
If there is a persistent ringing, whooshing, or buzzing in your ear, and you have also been told your blood pressure is high, it is reasonable to wonder whether the two are connected. The short answer is yes: high blood pressure can cause tinnitus, and the relationship between them is more direct than most people realize. But the details matter. Not all tinnitus linked to blood pressure is the same, and the type, timing, and character of the sound can tell a lot about what is happening and what to do next.
This guide explains the connection clearly, helps identify whether the ringing in your ears may be blood pressure-related, and outlines when to talk to a doctor.
Find a doctor near you if you are looking for a clinician who handles both cardiovascular and hearing health.
At a Glance
| Topic | Key Facts |
|---|---|
| Condition link | High blood pressure (hypertension) can damage the small blood vessels supplying the inner ear, leading to tinnitus |
| Types of tinnitus | Pulsatile (rhythmic, heartbeat-synced) and non-pulsatile (continuous ringing or buzzing); blood pressure most directly causes pulsatile tinnitus |
| Who is at risk | Adults with uncontrolled or long-standing hypertension; older adults with concurrent age-related hearing change |
| Co-occurrence | A peer-reviewed study in Frontiers in Neurology found hypertension was significantly more prevalent among tinnitus patients than among those without tinnitus |
| Reversibility | May improve with blood pressure control if cochlear damage has not yet become permanent; earlier treatment improves outcomes |
| When to seek urgent care | New-onset pulsatile tinnitus, sudden one-sided hearing loss, tinnitus with headache or neurological symptoms |
Why the Inner Ear Is Especially Vulnerable to Blood Pressure Changes
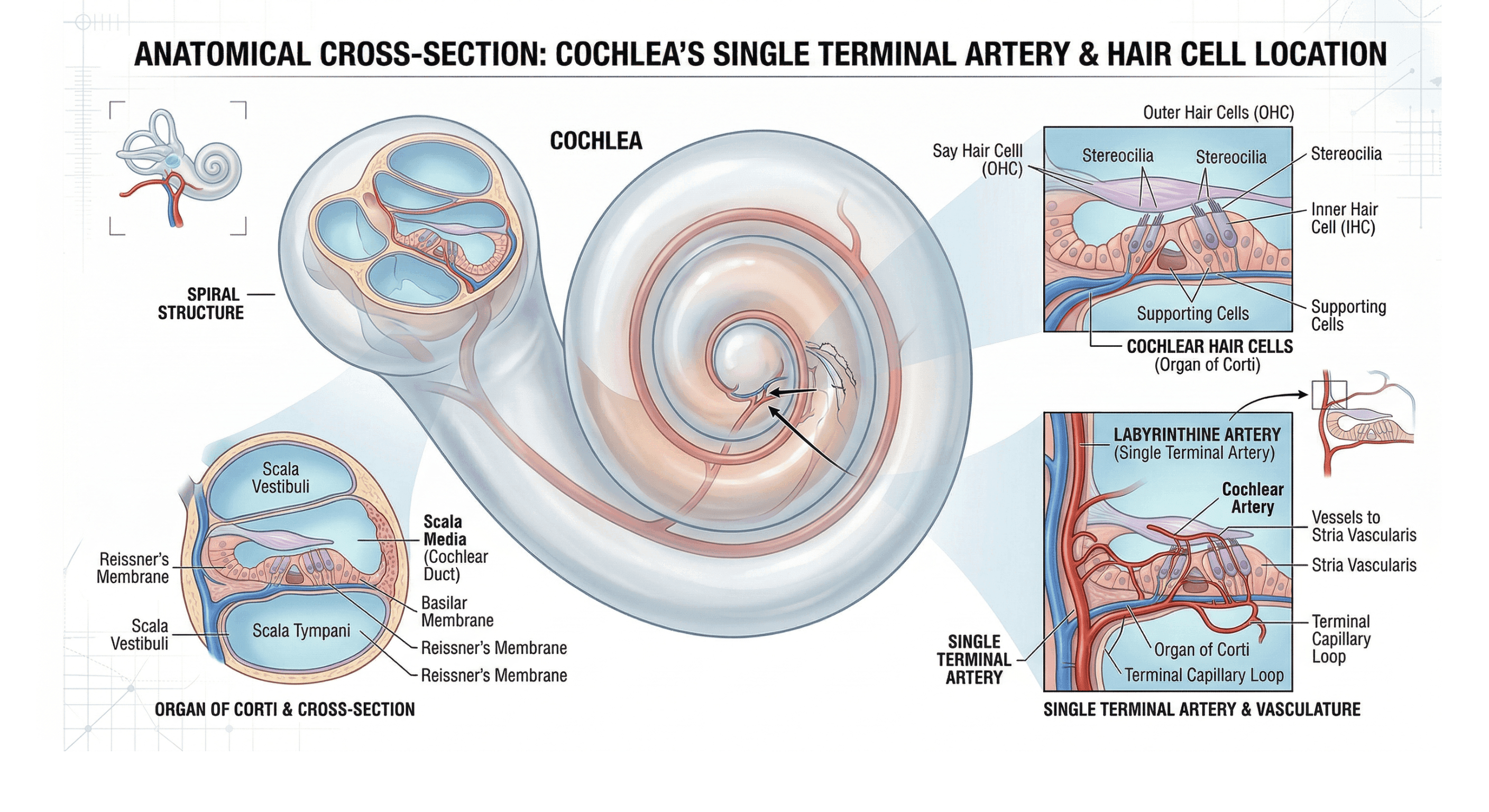
The cochlea, the spiral-shaped structure in the inner ear responsible for converting sound vibrations into nerve signals, has a notable anatomical characteristic: it is supplied by a single terminal artery with no backup blood supply. Most organs in the body have collateral circulation, meaning nearby vessels can compensate if one is compromised. The cochlea does not have that redundancy.
Even modest, sustained increases in blood pressure can reduce oxygen delivery to cochlear hair cells, the microscopic sensory cells that translate sound. Cochlear hair cells do not regenerate once damaged, which is why managing blood pressure early is more effective than waiting for symptoms to become established.
The Three Pathways Linking High Blood Pressure to Tinnitus
Three distinct mechanisms explain how high blood pressure generates or amplifies tinnitus:
1. Microvascular damage reducing cochlear perfusion. Sustained high pressure gradually damages the small capillaries feeding the cochlea, reducing blood flow and limiting the oxygen supply to hair cells. This is the slow, cumulative pathway most associated with long-standing hypertension.
2. Turbulent blood flow creating an audible vascular sound. When blood moves through narrowed or stiffened vessels near the ear with greater force, it can generate a sound the person can hear. This is typically described as a whooshing, pulsing, or thumping that beats in rhythm with the heart, and it is the mechanism behind pulsatile tinnitus.
3. Increased blood viscosity reducing oxygen delivery. High blood pressure is associated with thicker blood, which flows less freely through the fine capillaries of the inner ear. Reduced flow means less oxygen reaches cochlear structures. According to the National Institute on Deafness and Other Communication Disorders (NIDCD), circulatory problems are among the recognized causes of tinnitus.
Pulsatile Tinnitus vs. Regular Tinnitus: Why the Distinction Matters
Not all tinnitus is alike, and the difference is clinically relevant when blood pressure is involved.
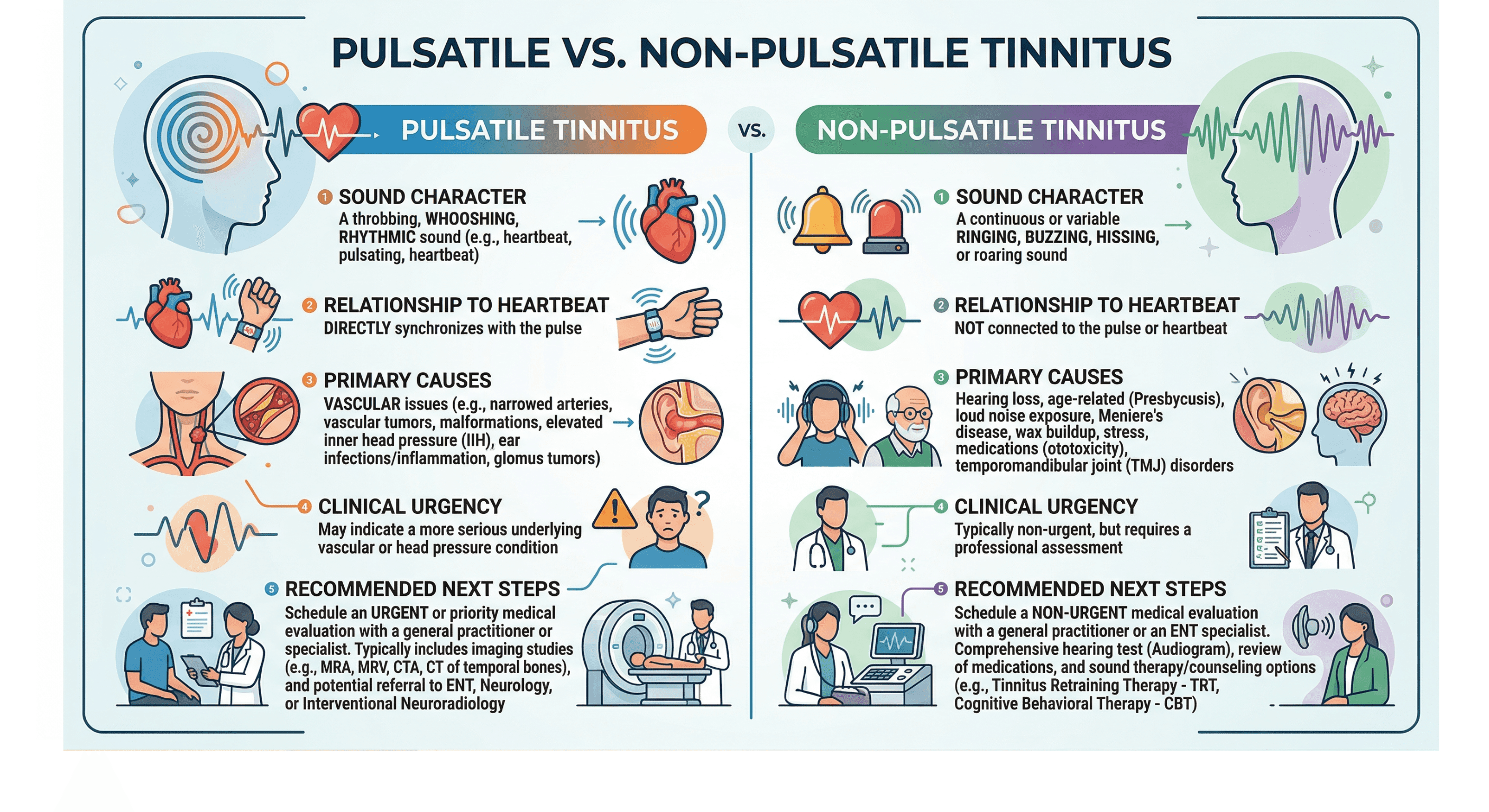
Non-pulsatile tinnitus is a continuous or near-continuous ringing, buzzing, hissing, or clicking. It tends to be steady, unrelated to heartbeat rhythm, and can have many causes including noise exposure, age-related hearing change, medication effects, and vascular disease.
Pulsatile tinnitus is a rhythmic sound, typically a whooshing, thumping, or pounding, that syncs with the heartbeat. It is specifically a vascular signal. When blood moves through narrowed or high-pressure vessels near the ear, the turbulence can become perceptible as sound.
High blood pressure most directly produces pulsatile tinnitus. According to the Mayo Clinic, conditions affecting blood vessels, including high blood pressure, atherosclerosis, and malformed vessels, can cause blood to move with greater force and produce tinnitus or make existing tinnitus more noticeable.
New-onset pulsatile tinnitus, particularly in one ear, should be assessed by a physician rather than assumed to be blood pressure-related. While hypertension is a common cause, a physician can also rule out other vascular contributors that benefit from early diagnosis.
How to Tell If Tinnitus May Be Blood Pressure-Related
There is no at-home test that confirms blood pressure as the cause of tinnitus. Several patterns, however, suggest the connection is worth exploring with a doctor:
| Signal | What it may suggest |
|---|---|
| Tinnitus began or worsened around the time of a hypertension diagnosis | Temporal correlation worth investigating |
| Sound is rhythmic and beats in time with the pulse | Strongly suggests vascular origin |
| Tinnitus fluctuates, louder during exertion, stress, or after salty meals | Possible BP-sensitive tinnitus |
| Tinnitus is in one ear only | Warrants evaluation to rule out structural causes |
| Tinnitus is in both ears | More consistent with systemic causes including hypertension |
| Ringing or buzzing started with a new blood pressure medication | Possible medication-related cause (see next section) |
A physician or audiologist can assess tinnitus character, conduct a hearing evaluation, and review blood pressure history to determine whether a vascular workup is appropriate. Find a doctor near you if these patterns are familiar.
Can Blood Pressure Medications Cause Tinnitus?
Some medications used to treat high blood pressure carry a potential for adverse effects on the auditory system, a property called ototoxicity. The classes most associated with tinnitus include:
- Loop diuretics (such as furosemide): Associated with tinnitus and hearing change primarily at high intravenous doses used in acute care settings. The low-to-moderate oral doses typically prescribed for hypertension management are considerably less likely to reach ototoxic thresholds. According to the American Academy of Audiology, ototoxic drug effects are dose-dependent and often reversible when the medication is adjusted.
- Aspirin at high doses: Daily low-dose aspirin (typically 81 mg) prescribed for cardiovascular prevention is generally below the dose threshold associated with tinnitus. High-dose aspirin has documented ototoxic potential, but this applies at doses far above standard cardiovascular prescriptions.
- Some beta-blockers and ACE inhibitors: Case reports exist, but the evidence for a consistent ototoxic effect from these classes is less robust.
If tinnitus began after starting or changing a blood pressure medication, that timeline is worth reporting to the prescribing physician. A medication review or dosage adjustment may be appropriate. Stopping blood pressure medication without medical guidance carries separate risks, and a doctor can advise on alternatives.
The Bidirectional Stress Loop: How Tinnitus Can Worsen Blood Pressure
The relationship between high blood pressure and tinnitus is not one-directional. Each condition can amplify the other through a stress pathway.
Chronic tinnitus, particularly when it disrupts sleep and concentration, activates the body's stress response. Elevated cortisol and adrenaline from chronic stress raise blood pressure and increase heart rate. Higher blood pressure, in turn, worsens cochlear perfusion and can intensify the tinnitus signal. The result is a self-reinforcing pattern where managing one condition without addressing the other may produce incomplete results.
According to the American Heart Association, chronic psychological stress is a recognized contributor to sustained blood pressure elevation. Stress reduction is not secondary in managing hypertension-related tinnitus; it is part of the overall treatment picture.
Will Tinnitus Go Away If Blood Pressure Is Controlled?
Whether tinnitus resolves with blood pressure control depends on the underlying cause and how long the cochlea has been under vascular stress.
- If tinnitus is driven by active high blood pressure and vascular turbulence, particularly pulsatile tinnitus, normalizing blood pressure often reduces or eliminates the sound. The turbulence driving the noise can resolve as vessel pressure drops.
- If tinnitus reflects early-stage cochlear perfusion change without permanent hair cell loss, meaningful improvement after blood pressure control is possible. According to the National Heart, Lung, and Blood Institute (NHLBI), effective blood pressure management through lifestyle changes and medication reduces the vascular stress that contributes to ear symptoms.
- If tinnitus reflects long-standing cochlear change from years of uncontrolled hypertension, blood pressure control at that stage may prevent further progression but may not fully reverse existing tinnitus. Sound therapy, hearing aids with tinnitus masking features, or cognitive behavioral therapy (CBT) become more relevant in those cases.
Treating blood pressure early, before permanent cochlear change occurs, gives the best chance of tinnitus improvement.
Managing Both Conditions: What the Evidence Supports
Effective management of hypertension-related tinnitus generally requires addressing both conditions. A doctor can advise on what applies to an individual case, but the evidence-supported approaches include:
Addressing blood pressure directly:
- Blood pressure monitoring and medication as prescribed
- The DASH (Dietary Approaches to Stop Hypertension) diet, which according to the NHLBI has been shown to reduce systolic blood pressure in clinical studies
- Sodium restriction, as dietary sodium is a modifiable driver of blood pressure elevation
- Regular aerobic exercise; the American College of Cardiology notes that 150 minutes of moderate exercise per week is associated with meaningful blood pressure reduction
Addressing tinnitus directly:
- Sound therapy and masking: White noise machines or masking devices can reduce the perceptibility of tinnitus, particularly for sleep disruption
- Tinnitus Retraining Therapy (TRT): A structured behavioral approach that combines sound therapy with counseling to reduce the brain's attentional response to tinnitus signals; according to the American Tinnitus Association, TRT has demonstrated benefit in clinical studies for reducing tinnitus distress
- Cognitive Behavioral Therapy (CBT): Addresses the anxiety and heightened attention that amplify tinnitus perception; shown in multiple studies to reduce tinnitus-related distress even when the sound itself persists
- Hearing aids with tinnitus masking features: When hearing loss is also present, amplification can reduce tinnitus perception by restoring ambient sound
Use Momentary Lab's AI healthcare navigator to identify which specialists handle the overlap between cardiovascular and hearing health.
When Tinnitus With High Blood Pressure Needs Prompt Attention
Most tinnitus associated with high blood pressure does not require emergency care. Certain symptom combinations, however, do warrant prompt evaluation.
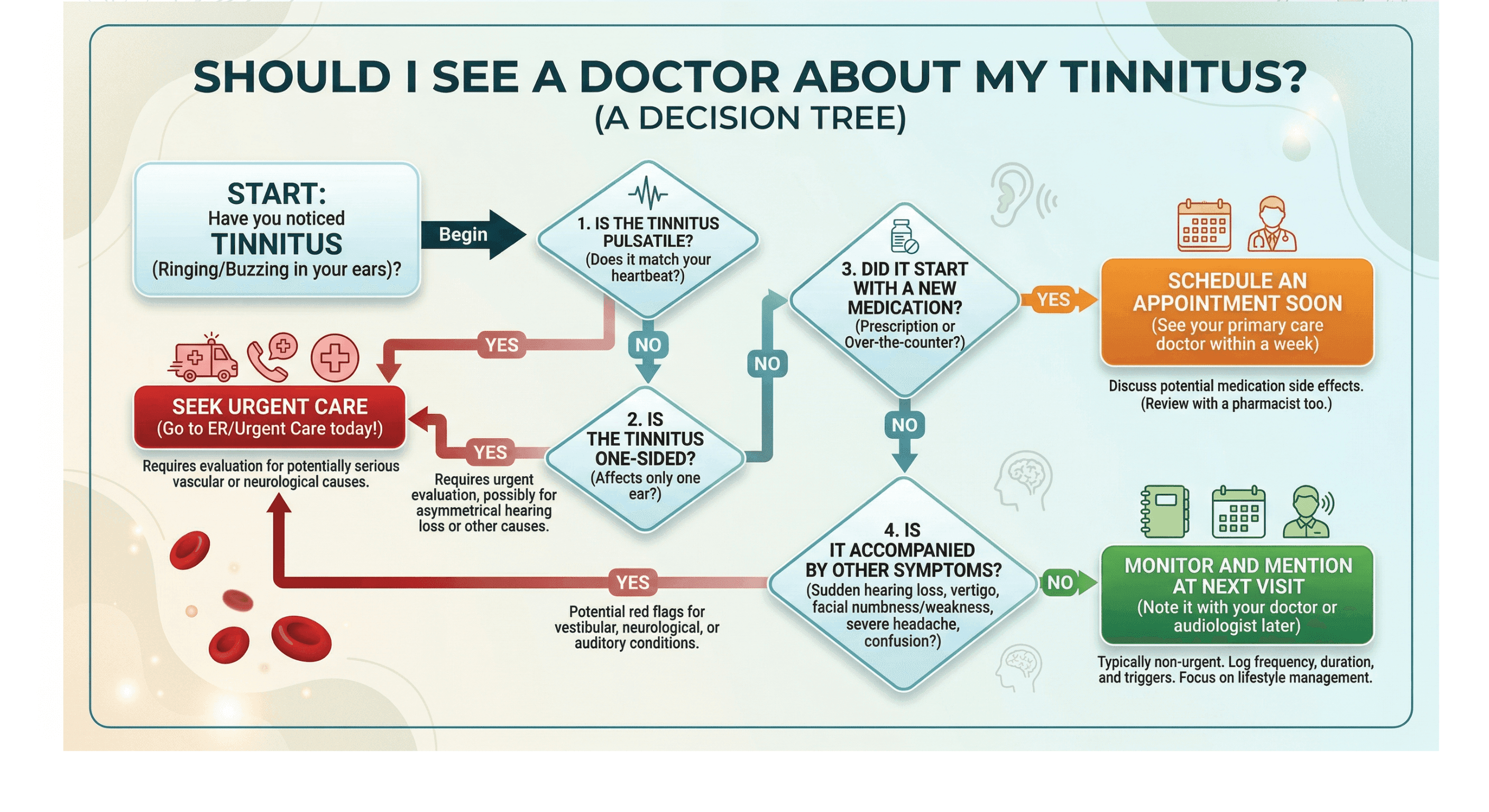
Seek same-day or urgent care if:
- Tinnitus is new, pulsatile (heartbeat-synced), and one-sided; this combination should be evaluated with imaging to rule out a vascular cause
- Tinnitus is accompanied by sudden hearing loss in one ear; sudden sensorineural hearing loss is a time-sensitive condition where early treatment improves outcomes
- Tinnitus is accompanied by severe headache, visual disturbance, or limb weakness; these symptoms together warrant emergency evaluation
Schedule a prompt, non-emergency appointment if:
- Tinnitus began or significantly worsened at the same time as a blood pressure diagnosis or medication change
- Tinnitus has been present for more than two weeks and has not been previously evaluated
- Tinnitus is affecting sleep, concentration, or daily function
A primary care physician can conduct an initial assessment and refer to an audiologist, ENT, or vascular specialist as appropriate. Find a doctor near you.
Frequently Asked Questions
Can lower blood pressure reduce tinnitus?
Lowering blood pressure can reduce tinnitus in some cases, particularly when the tinnitus is pulsatile and driven by active vascular turbulence near the ear. When the primary mechanism is excess blood pressure forcing turbulent flow through vessels adjacent to the cochlea, reducing that pressure can reduce or resolve the sound. Improvement is more likely when blood pressure control is achieved before permanent cochlear hair cell damage has occurred. A doctor can evaluate whether blood pressure management is likely to influence an individual's tinnitus based on its character, duration, and associated hearing history.
What is the latest treatment for tinnitus?
As of 2025, tinnitus treatment remains symptom-focused rather than curative. The most evidence-supported approaches include Cognitive Behavioral Therapy (CBT), Tinnitus Retraining Therapy (TRT), and sound-based masking. According to the American Tinnitus Association, research into neuromodulation, including transcranial magnetic stimulation (TMS) and bimodal auditory-somatosensory stimulation, is ongoing, with some studies showing modest benefit in reducing tinnitus loudness and distress. The FDA granted De Novo authorization to one bimodal stimulation device (Lenire) for tinnitus relief in 2022. Response varies by individual, and a physician or audiologist can advise on which approach fits a specific case.
What can cause tinnitus to flare up?
Tinnitus intensity can increase in response to several triggers. High salt intake can temporarily raise blood pressure and fluid pressure in the inner ear, worsening the sound. Caffeine and alcohol, both of which affect vascular tone, are commonly reported tinnitus amplifiers. Psychological stress activates the sympathetic nervous system, raising blood pressure and heightening the brain's sensitivity to internal sounds. Loud noise exposure causes temporary threshold shifts that make tinnitus more prominent. Poor sleep reduces the brain's ability to suppress tinnitus signals. For people with hypertension-related tinnitus, uncontrolled blood pressure spikes are a particularly direct trigger.
What does high blood pressure sound like in your ears?
Hypertension-related tinnitus most commonly presents as a pulsing, whooshing, or thumping sound that beats in time with the heartbeat. This is called pulsatile tinnitus, and it reflects turbulent blood flow in vessels near the cochlea. Some people describe it as a rushing or pumping sensation rather than a tone. Non-pulsatile tinnitus, a steady ringing or buzzing, can also be associated with high blood pressure through the longer-term mechanism of cochlear blood flow reduction, though this presentation is harder to attribute specifically to blood pressure without clinical evaluation.
The Bottom Line
High blood pressure can cause tinnitus through three overlapping mechanisms: microvascular damage to the cochlea, turbulent blood flow producing audible vascular sounds, and reduced oxygen delivery from increased blood viscosity. The cochlea's lack of collateral circulation makes it particularly sensitive to vascular stress.
Pulsatile tinnitus, a rhythmic sound synced to the heartbeat, is the presentation most directly linked to blood pressure and warrants evaluation to address hypertension and rule out other vascular contributors.
Whether tinnitus improves with blood pressure control depends on how early treatment begins and whether cochlear change has become permanent. Acting on hypertension-related ear symptoms early is clinically meaningful.
A physician can assess the relationship between blood pressure and tinnitus in an individual case and determine whether additional evaluation by an audiologist, ENT, or vascular specialist is appropriate. Find a doctor near you.



