
If your knee replacement feels wobbly, makes new clicking or clunking noises, or has started hurting again years after surgery, the fear that something is seriously wrong is legitimate. And the question that follows is immediate: does this mean going back to the operating room?
The short answer is: it depends on why the implant feels loose. True mechanical loosening, where the implant has physically detached from the bone, cannot be corrected without surgery. But a significant share of patients who report a "loose" knee actually have functional instability, a condition involving the surrounding soft tissue and muscle rather than the implant itself. That distinction changes everything, including whether surgery is even on the table.
This guide walks through both scenarios with clarity, covers the diagnostic process your surgeon will likely follow, and gives a practical framework for figuring out your next step.
At a Glance
| Topic | Key Facts |
|---|---|
| Primary keyword condition | Mechanical loosening of a total knee replacement (TKR) |
| Most common cause of revision surgery | Aseptic loosening and instability |
| Can non-surgical care fix true loosening? | No. It can manage symptoms but cannot reattach the implant |
| Can non-surgical care fix functional instability? | Yes, in many cases |
| First step if you suspect loosening | Orthopedic evaluation with X-ray and infection labs |
| Red flag requiring urgent care | Fever, drainage, or sudden severe joint collapse |
| Primary surgical fix | Revision total knee arthroplasty (TKA) |
The Short Answer: What Non-Surgical Care Can and Cannot Do
Patients hoping to avoid a return to the OR deserve a straight answer before anything else.
Non-surgical treatments cannot reattach an implant that has mechanically separated from the bone. No brace, no injection, and no amount of physical therapy changes the underlying structural problem once the bond between implant and bone has failed. What non-surgical care can do is reduce pain, improve function, and slow symptom progression while you and your surgeon decide on timing. For patients with functional instability rather than true loosening, conservative care is often a complete and appropriate treatment path.
The medical reality is that the category of loosening you have determines every decision downstream. Getting that diagnosis right is the most important thing that happens before any treatment begins.
Not All "Loose" Knee Replacements Are the Same
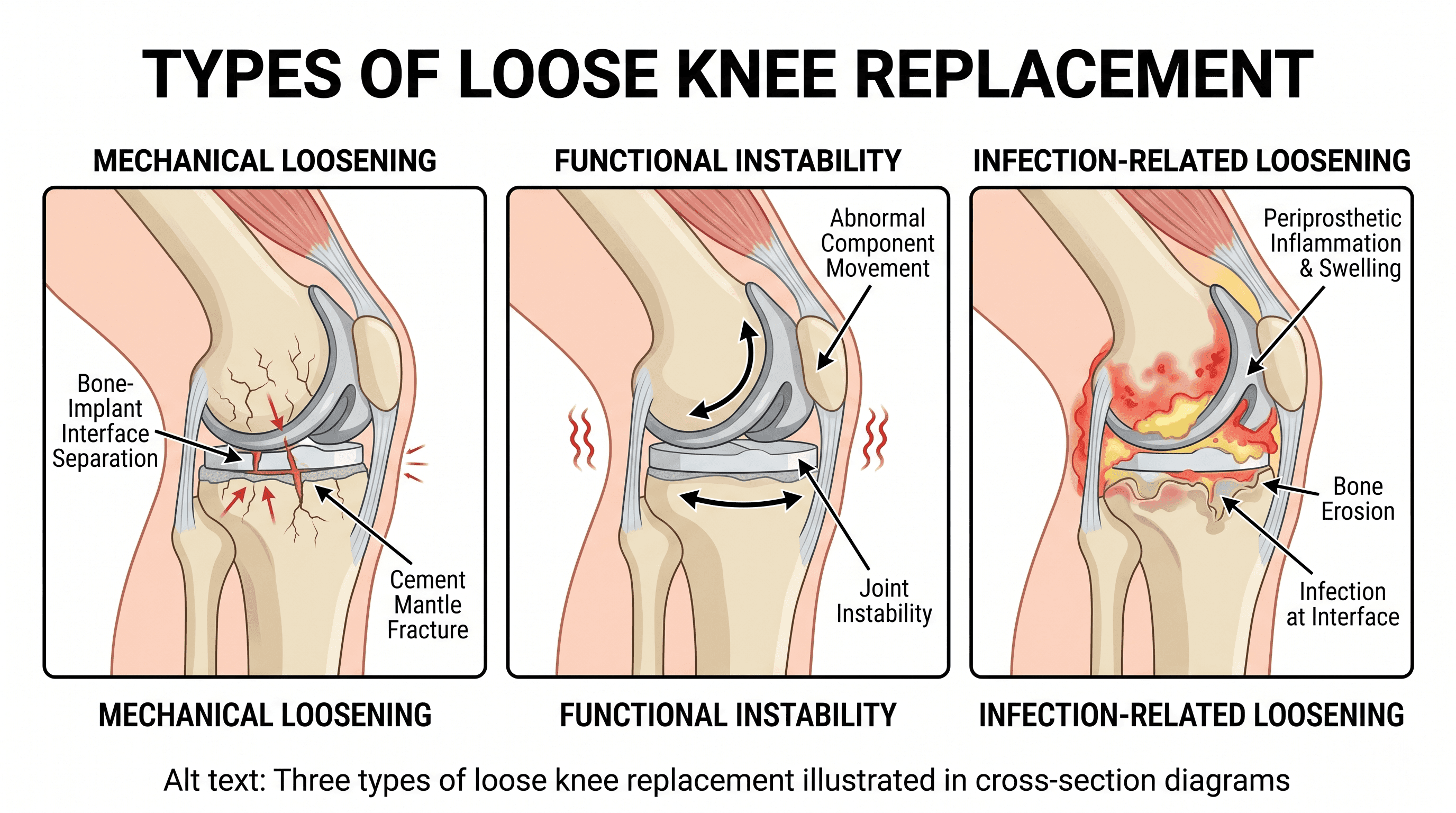
The word "loose" gets used loosely, and that creates real confusion. Orthopedic surgeons distinguish between three separate clinical scenarios that patients and even some general practitioners often conflate.
True Mechanical Loosening: When the Implant Detaches
Mechanical loosening, also called aseptic loosening when infection is not the cause, refers to the physical failure of the bond between the implant and the surrounding bone. In cemented implants, the bone cement breaks down. In cementless implants, the bone that was expected to grow into the implant surface fails to do so adequately, or gradually pulls away.
According to the AAOS OrthoInfo resource on revision total knee replacement, loosening and instability are among the most common reasons patients require revision surgery. Aseptic loosening is consistently identified as a leading driver of long-term implant failure.
A separate process called osteolysis, or bone loss around the implant, frequently accompanies mechanical loosening. Tiny particles shed by a wearing implant trigger an immune response that gradually erodes the surrounding bone. This creates a vicious cycle: bone loss makes the implant less stable, which accelerates wear, which produces more particles. Non-surgical care cannot interrupt this cycle. It requires surgical intervention.
Functional Instability: When the Implant Is Fine but the Knee Is Not
Functional instability is a different condition entirely. The implant itself remains properly bonded to the bone, but the knee feels unstable or "gives way" because of problems in the surrounding soft tissue, including stretched or weakened ligaments, muscle weakness in the quadriceps, hamstrings, or glutes, post-operative scar tissue, or persistent swelling that alters joint mechanics.
This is the category where physical therapy, bracing, and activity modification can produce genuine improvement. Patients with functional instability are often misled by the term "loose" into assuming they need revision surgery when they actually need a structured rehabilitation program.
Infection-Related Loosening: The Scenario to Rule Out First
A late-onset infection around the implant, called periprosthetic joint infection (PJI), can cause symptoms nearly identical to mechanical loosening. Pain, swelling, and a sense of instability all appear. But the treatment pathway is completely different and significantly more aggressive. Ruling out infection is always the first clinical priority before any other cause is investigated. This is not optional and is not negotiable as a diagnostic step.
What a Loose Knee Replacement Actually Feels Like
Signs of a loose knee implant vary depending on the underlying cause, but several symptoms appear consistently across cases.
Pain that returns after a period of relief is often the first signal. Many patients describe a honeymoon period of several years with no significant discomfort, followed by the gradual return of pain, particularly during weight-bearing or at the start of movement after rest. This "start-up pain" pattern is a recognized hallmark of implant loosening and is worth mentioning specifically to a surgeon.
A feeling of instability or giving way is another common report, and this is where the distinction between mechanical loosening and functional instability becomes practically important. Giving way associated with mechanical loosening tends to occur unpredictably and under load. Giving way from functional instability more often correlates with specific movements, like descending stairs or pivoting, where the supporting muscles are taxed.
Knee popping years after surgery, or new clunking and grinding sounds, can reflect implant micromotion or component wear. Swelling that appears without a clear injury trigger is also worth noting, as is visible deformity or a shift in how the leg is aligned compared to how it looked shortly after the original surgery.
Red Flag Signs That Require Seeing a Surgeon This Week
Some symptoms indicate a situation serious enough to warrant prompt surgical evaluation rather than a scheduled routine appointment. Contact an orthopedic surgeon urgently if any of the following are present.
Fever above 101 degrees Fahrenheit accompanied by knee pain or swelling suggests possible infection. Warmth, redness, and drainage from the incision site, even years after the original surgery, also indicate potential infection and require immediate evaluation. A sudden, dramatic spike in pain without a clear injury cause, especially if accompanied by an inability to bear weight, warrants same-week or same-day contact with a surgeon. Any visible deformity or frank joint collapse, meaning the knee buckles or locks in a position it has not held before, is an urgent presentation.
These scenarios require evaluation because conservative management alone cannot address the underlying cause, and delay in the setting of infection or severe bone loss can significantly complicate any future surgical repair.
How Doctors Diagnose a Loose Knee Replacement
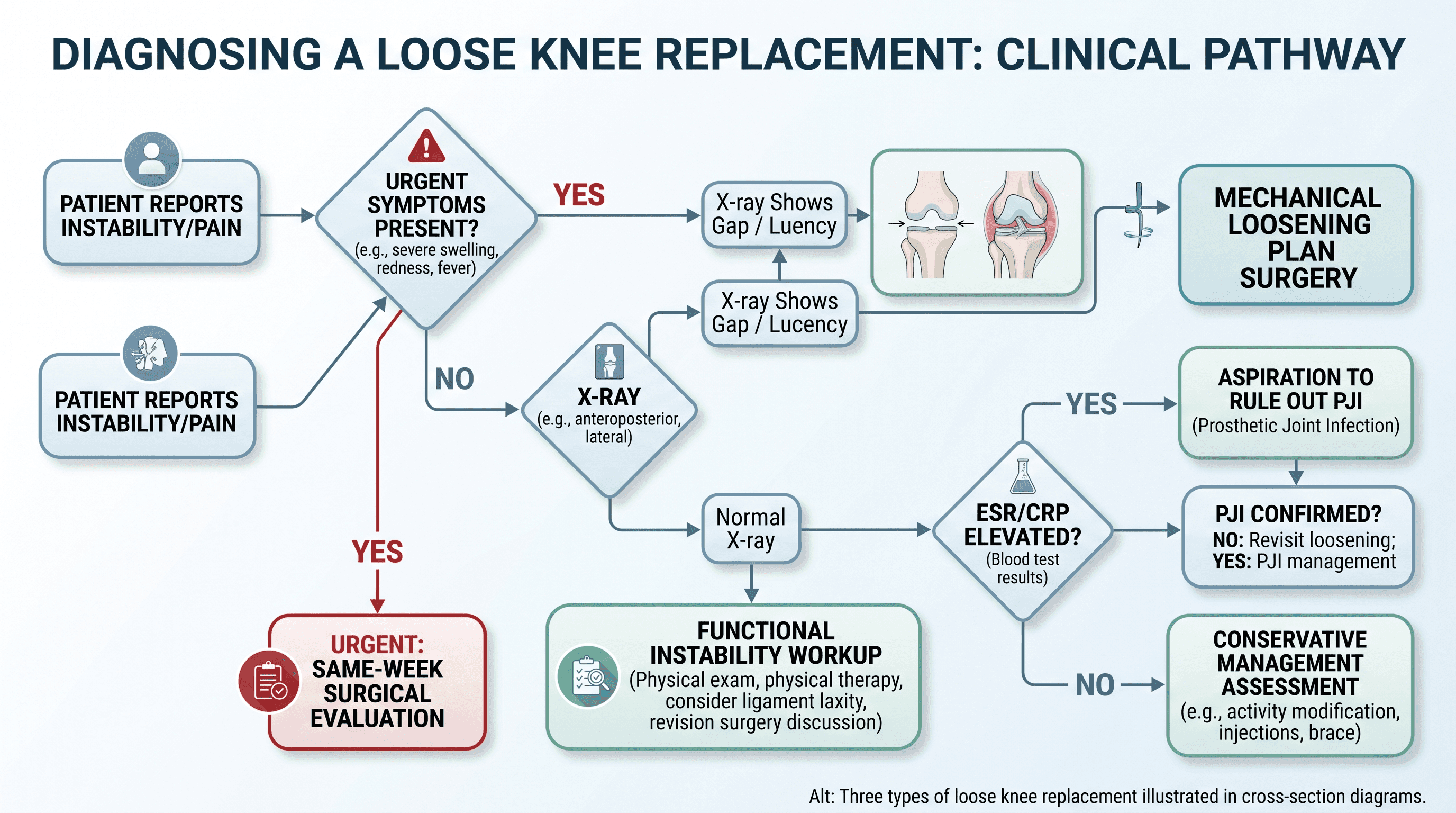
The diagnostic process for a suspected loose knee implant follows a clear sequence, and understanding it takes some of the anxiety out of the first appointment.
X-rays are almost always the starting point. Weight-bearing X-rays can reveal a visible gap or radiolucent line between the implant and the bone, which indicates loosening. Component alignment and any visible bone loss around the implant are also assessed on plain films. In many cases, X-rays provide enough information to confirm or rule out mechanical loosening.
Blood tests measuring inflammatory markers, specifically erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), are ordered when infection is on the differential. These markers are elevated in most cases of periprosthetic joint infection and serve as a screen before more invasive testing.
Joint aspiration involves drawing fluid from the knee joint for laboratory analysis. It provides the most direct evidence of infection and can help characterize the nature of any inflammatory process occurring inside the joint. Bone scans using radioactive tracers can detect abnormal bone activity around the implant that standard X-rays may miss in early-stage loosening. CT or MRI imaging offers additional detail when the surgeon needs precise information about bone stock or soft tissue involvement before planning a surgical approach.
Non-Surgical Options: What Can Legitimately Help and What Cannot
Non-surgical management of a loose knee replacement is most effective for patients with confirmed functional instability. For patients with confirmed mechanical loosening, these approaches manage symptoms but do not address the structural problem.
Physical Therapy: Strengthening the Right Muscles
A targeted physical therapy program for functional instability focuses on the quadriceps, hamstrings, and gluteal muscles, all of which contribute to knee joint stability. Stronger surrounding musculature reduces the load transferred to the implant-bone interface and can meaningfully reduce the feeling of giving way.
Physical therapy is appropriate when imaging confirms the implant is intact and when functional instability is the primary diagnosis. It is not appropriate as a standalone response to confirmed mechanical loosening, and using it as such risks delaying a necessary surgical intervention while bone loss progresses.
Bracing: Support Versus Long-Term Dependence
Knee bracing can reduce pain and improve confidence during ambulation, particularly for patients who are waiting for surgical scheduling or those managing functional instability. Rehabilitative braces and unloader braces serve somewhat different purposes, and a surgeon or physical therapist can advise on which type fits a specific presentation.
A practical caution: long-term reliance on bracing as the primary management strategy for mechanical loosening can mask worsening symptoms and create a false sense of stability while the underlying implant failure progresses. Bracing works best as a temporary bridge, not a permanent solution.
Activity Modification and Weight Management
High-impact activities, including running, jumping, and heavy lifting, place forces on the knee implant that accelerate wear and can worsen loosening over time. Reducing these activities is one of the few conservative measures that directly influences the mechanical environment around the implant rather than just managing symptoms.
Weight management has a measurable impact on implant longevity. Research published in PMC has examined the relationship between body mass index and revision rates after total knee arthroplasty, with excess weight associated with higher complication rates and accelerated implant stress. Even modest weight reduction can reduce joint load substantially.
Pain Management: Anti-Inflammatories and Injections
NSAIDs such as ibuprofen and naproxen are commonly used to manage pain in patients with implant-related discomfort. Corticosteroid injections offer targeted short-term inflammation relief but carry risks with repeated use, including potential weakening of periarticular tissue. Platelet-rich plasma (PRP) injections have been explored for various knee conditions, but evidence supporting their use specifically in the context of knee replacement loosening remains limited and inconclusive at this time.
All of these approaches treat symptoms rather than causes. A doctor can advise on which, if any, are appropriate given an individual patient's diagnosis and overall health profile.
The Dangers of Waiting
Delaying evaluation and treatment for a suspected loose knee implant is not a neutral choice. In cases of mechanical loosening accompanied by osteolysis, bone loss around the implant progresses over time. The more bone that is lost before revision surgery, the more complex the reconstruction becomes.
Surgeons performing revision procedures with significant bone loss must use bone grafts or specialized augmented implant components to restore the structural environment around the new implant. These procedures are longer, carry higher complication rates, and have lower long-term success rates compared to revisions performed before bone stock is severely compromised. Research published in PMC on complications and revisions following total knee arthroplasty underscores how the timing of intervention affects surgical complexity and outcomes.
In the setting of infection, delay carries additional risk of systemic spread. Periprosthetic joint infections can track along fascial planes and are significantly harder to eradicate once they are established. Early identification and treatment improve outcomes markedly.
Facing the Inevitable: An Overview of Revision Knee Surgery
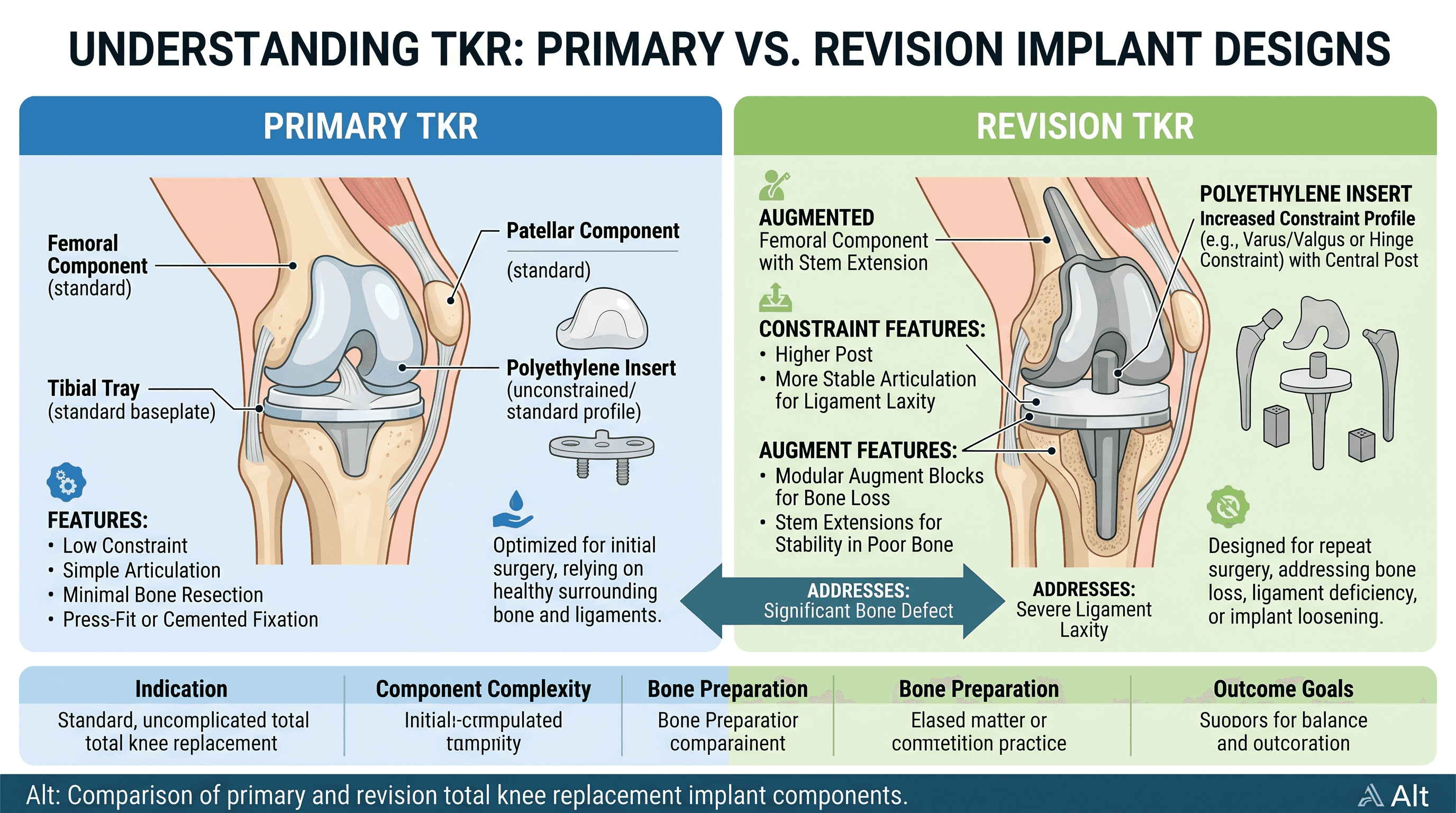
Revision total knee arthroplasty is more complex than primary knee replacement, but it is also a well-established procedure with good outcomes in appropriately selected patients. Understanding what it involves can reduce the anxiety that often surrounds the prospect of returning to surgery.
Revision surgery involves removing the existing implant components, cleaning the bone surfaces, addressing any bone loss with graft material or metal augments, and implanting a new set of components designed specifically for revision situations. Revision implants are typically more constrained than primary implants, meaning they incorporate more structural stability into the implant design itself to compensate for any ligamentous laxity.
The scope of the revision depends on which components have failed. In some cases, only one component, such as the tibial insert, requires replacement. In others, both the femoral and tibial components must be removed and replaced.
If you are approaching a decision about revision surgery, consulting with an experienced revision orthopedic specialist is an important step. Find a board-certified orthopedic surgeon near you through Momentary Lab's doctor directory to get a specialist evaluation and a second opinion if needed.
What to Expect From Recovery
Recovery from revision knee replacement is typically longer and more demanding than recovery from a primary knee replacement. Most patients begin physical therapy within a few days of surgery and can expect to use a walker or crutches for several weeks. Return to independent walking without an assistive device generally occurs within six to twelve weeks for uncomplicated revisions. Return to more demanding activities takes several months, and full functional recovery may take up to a year.
Realistic expectations, consistent physical therapy participation, and close communication with the surgical team are the most reliable predictors of a good outcome.
How Long Will the Revision Last?
Revision implants have lower long-term survival rates than primary implants, but outcomes are improving steadily as implant design and surgical technique advance. A large meta-analysis published in Nature Scientific Reports examining total knee arthroplasty survival data reflects the substantial body of evidence supporting the long-term durability of knee replacement procedures. Revision implants benefit from ongoing improvements in materials and fixation methods, and many patients achieve durable results that last well over a decade.
The most important predictor of revision implant longevity is the condition of the bone stock at the time of surgery, which is one of the clearest reasons why timely evaluation and treatment matter.
Your Decision Framework: A Step-by-Step Patient Guide
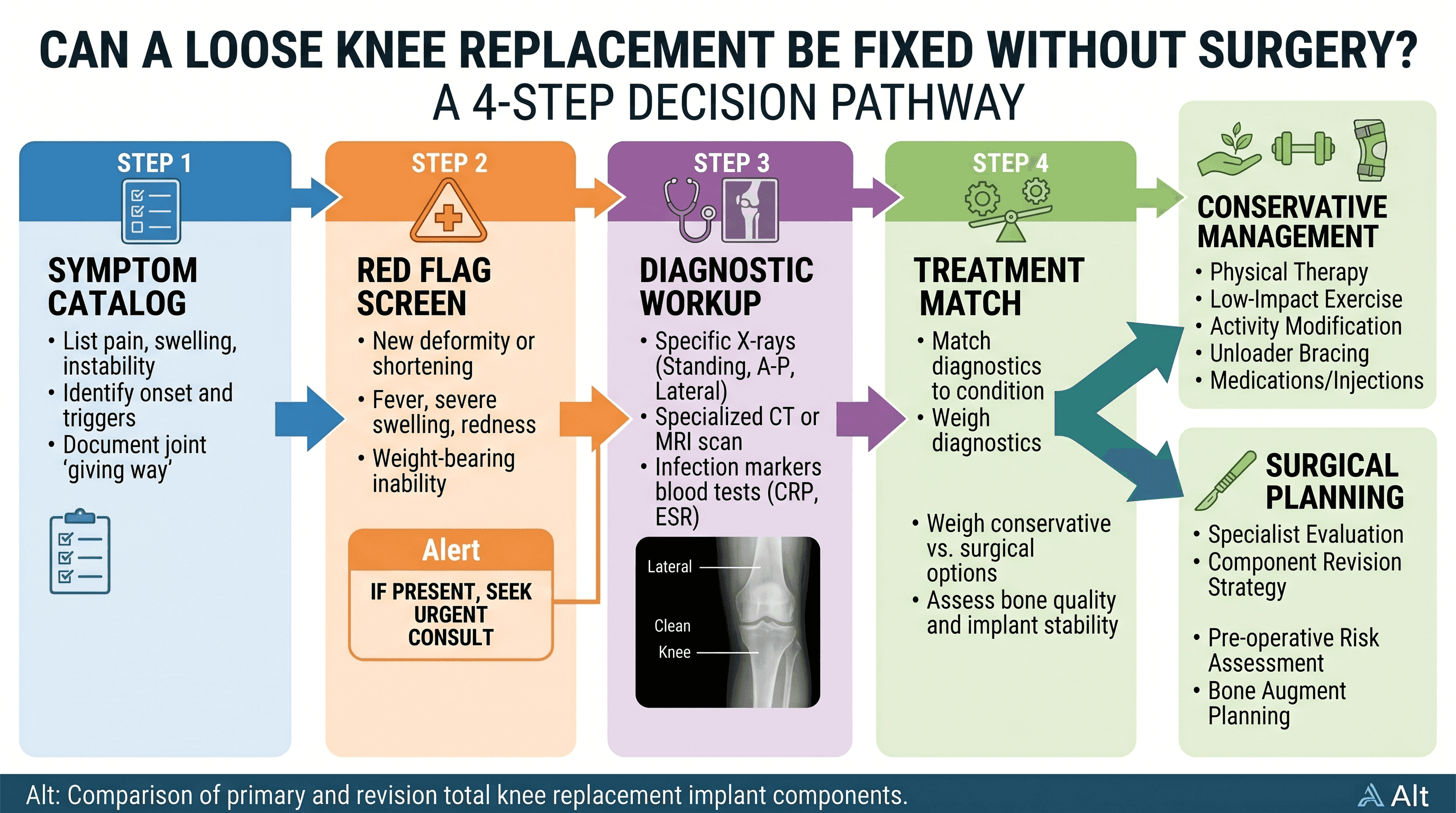
Patients facing a potential knee replacement failure benefit from a clear pathway rather than a list of options. Here is a four-step framework.
Step 1: Catalog your symptoms. Note when pain started, whether it is at rest or with weight-bearing, whether the knee gives way, and any new sounds or visible changes. Write these down before the appointment.
Step 2: Screen for red flags. If fever, drainage, sudden severe pain, or complete joint instability are present, contact a surgeon this week rather than scheduling a routine appointment.
Step 3: Get a complete diagnosis. Request weight-bearing X-rays, inflammatory markers, and, if infection is suspected, joint aspiration. Do not accept a management plan before the category of loosening is confirmed.
Step 4: Match your diagnosis to a treatment path. Functional instability without mechanical loosening warrants a structured physical therapy trial. Confirmed mechanical loosening, osteolysis, or infection requires surgical planning. The timing of that surgery depends on symptom severity, rate of bone loss, and the patient's overall health.
Questions to Ask Your Orthopedic Surgeon
Walking into a surgical consultation armed with specific questions produces better outcomes than a general conversation about symptoms. Consider asking the following during the appointment.
Ask whether the issue is mechanical loosening or functional instability, and request that the distinction be explained in terms of what the imaging shows. Ask which specific components appear to be involved if loosening is confirmed. Ask whether infection has been ruled out and by what testing. If revision surgery is recommended, ask whether all components need to be replaced or only specific ones. Ask about the surgeon's revision volume, since higher-volume revision surgeons consistently achieve better outcomes in published literature. Ask what happens if surgery is delayed by three to six months, since this gives insight into how urgently the loosening needs to be addressed based on the rate of bone loss. Ask what the realistic functional outcome looks like after recovery, including return to specific activities that matter most to daily life.
These questions position the patient as an informed participant rather than a passive recipient of a treatment plan. For additional guidance on navigating your healthcare options, the Momentary Lab AI Healthcare Navigator can help with finding care, understanding conditions, and preparing for specialist appointments.
Frequently Asked Questions
Can you walk with a loose knee replacement?
Many patients with a loose knee replacement can still walk, particularly in the early stages of loosening or when functional instability rather than mechanical failure is the primary problem. However, walking on a mechanically loose implant accelerates bone loss and implant wear over time. Continued ambulation without evaluation is not advisable once loosening is suspected, and any significant pain, instability, or giving way during walking warrants prompt orthopedic consultation.
What are the common causes of a loose knee replacement?
Aseptic loosening, meaning loosening not caused by infection, is the most frequently cited cause of long-term knee replacement failure. It typically results from gradual breakdown of the cement-bone or implant-bone interface over years of use. Osteolysis driven by implant wear particles is a closely related mechanism. Late-onset periprosthetic joint infection is a separate but important cause that requires different treatment. Functional instability caused by soft tissue laxity or muscle weakness is not true loosening but produces similar-feeling symptoms.
What is the newest alternative to knee replacement?
For patients who have not yet undergone knee replacement, options such as high tibial osteotomy, partial knee replacement, and cartilage restoration procedures are available depending on the pattern of arthritis and joint anatomy. Biologics and regenerative approaches are under active research. For patients with an existing knee replacement that is failing, however, revision total knee arthroplasty remains the primary and most established surgical intervention. A doctor can advise on whether any non-replacement alternatives apply to an individual case.
How can you tell if a knee replacement is loose?
The most common signs include the return of pain after a symptom-free period, a sensation that the knee gives way or wobbles during weight-bearing, new clicking or clunking noises, and swelling without an injury cause. However, these symptoms can also reflect functional instability or other conditions. A definitive diagnosis requires imaging, most often weight-bearing X-rays, combined with blood tests to rule out infection. Self-diagnosis is not reliable for this condition.
How can a loose knee joint be tightened without surgery?
If the looseness is functional instability rather than mechanical implant failure, strengthening the surrounding musculature through physical therapy can significantly reduce the feeling of instability. Bracing provides additional external support. Neither of these approaches tightens a mechanically loose implant or reverses osteolysis. For true mechanical loosening, there is no non-surgical method of reattaching the implant to the bone.
References
- PMC (PMC4061408) — Data on complications and revisions following total knee arthroplasty, cited for context on timing of intervention and surgical complexity.
- Nature Scientific Reports (s41598-024-71256-y) — Meta-analysis data on long-term survival and outcomes in total knee arthroplasty, cited for revision implant longevity discussion.
- PMC (PMC10010196) — Research on body mass index and revision rates after TKA, cited for weight management and implant stress discussion.
- AAOS OrthoInfo: Revision Total Knee Replacement — Clinical overview of causes of revision surgery and implant failure categories, cited for aseptic loosening and instability as leading revision drivers.
- PMC (PMC10898804) — Supporting clinical literature on knee arthroplasty outcomes and failure mechanisms.
- PMC (PMC7068007) — Additional clinical research on periprosthetic complications following total knee replacement.



