
If you've already been through one meniscus surgery and your knee is hurting again, the question sitting in your mind is probably a loaded one. You want a straight answer, but you also want to know what that answer actually means for your knee, your recovery, and your life going forward. This guide is written for exactly that situation.
At a Glance
| Topic | Key Facts |
|---|---|
| Can you have meniscus surgery twice? | Yes, in most cases a second surgery is possible |
| Most common reason for repeat surgery | Re-tear or failed healing after the first repair |
| Second surgery types | Revision repair, partial meniscectomy, or meniscal allograft transplant |
| Key candidacy factor | Remaining tissue quality, not age alone |
| Biggest long-term risk | Accelerated osteoarthritis after repeated cartilage removal |
| Recovery after second surgery | Typically longer than the first, especially after revision repair |
Yes, But It Depends on What Is Left
The direct answer is yes. A second meniscus surgery on the same knee is both medically possible and, in many cases, the appropriate next step. But the type of surgery recommended depends entirely on what the surgeon finds when evaluating your knee: how much meniscal tissue remains, whether the remaining tissue is healthy enough to repair, the condition of the surrounding cartilage, and what caused the problem to return in the first place.
This is not a simple repeat of whatever was done the first time. The second procedure might be the same approach, a completely different one, or in some cases, a discussion about whether surgery is the right path at all. Understanding the difference between those paths is where this guide begins.
Why Did It Tear Again? Causes of a Recurrent Meniscus Tear
Returning to the surgeon's office with a painful knee after meniscus surgery is more common than most patients expect. Before any decision about a second procedure is made, the root cause of the recurrence needs to be identified. The treatment pathway branches depending on whether the problem is a new traumatic tear, a failure of biological healing, or something related to how rehabilitation was managed.
Re-Tear vs. Failed Healing: Two Different Problems
A traumatic re-tear happens when the repaired or remaining meniscus is physically torn again, typically during activity. This is more common in younger, active patients who return to pivoting sports or heavy loading. It presents like the original injury: sudden pain, swelling, and mechanical symptoms such as locking or catching in the joint.
Failed healing is a different situation. In this case, the sutures from a prior repair may have held structurally, but the tissue never biologically integrated. The repair site remains a zone of weakness that degenerates over time. A 2021 systematic review published on PubMed noted that meniscus repair carries a measurable long-term failure rate, with failed healing being a distinct failure mode from mechanical re-tear.
The Red Zone vs. White Zone: Why Blood Supply Shapes the Odds
The meniscus is not uniformly vascularized. The outer third, called the red zone, has adequate blood supply to support biological healing after repair. The inner two-thirds, called the white zone, receives nutrients through diffusion only, making healing biologically unreliable after repair.
This anatomy matters enormously for second surgery decisions. A tear located in the white zone that was repaired the first time may have always had poor healing potential, regardless of surgical technique. According to research cited by the Mayo Clinic, approximately 70 to 75 percent of the meniscus lacks direct blood supply, which limits the tissue's natural ability to heal after injury.
Other Causes: Infection, Poor Rehab, and Returning Too Soon
A small percentage of failed meniscus repairs involve post-surgical infection or mechanical complications from the repair hardware. More commonly, however, modifiable factors play a role. Returning to high-impact activity before the tissue has sufficiently healed, skipping or shortening physical therapy, or having unaddressed alignment or ligament instability in the knee can all set up a repair for failure. If any of these factors contributed to the first failure, they need to be corrected before a second surgery proceeds.
A Second Meniscectomy: What Happens When There Is Less Cartilage Left?
When repair is not possible, the standard approach is a partial meniscectomy, meaning the surgeon trims away the damaged or unstable portion of the meniscus. A second partial meniscectomy on the same knee removes additional tissue, and that loss of cartilage volume carries real mechanical consequences.
The meniscus functions as a load-distributing shock absorber between the femur and tibia. Each millimeter of tissue removed increases the peak contact stress on the articular cartilage. Research published via PubMed demonstrated that even partial meniscal removal significantly increases joint contact pressures, a finding that underpins why repeat trimming is approached conservatively by experienced knee surgeons.
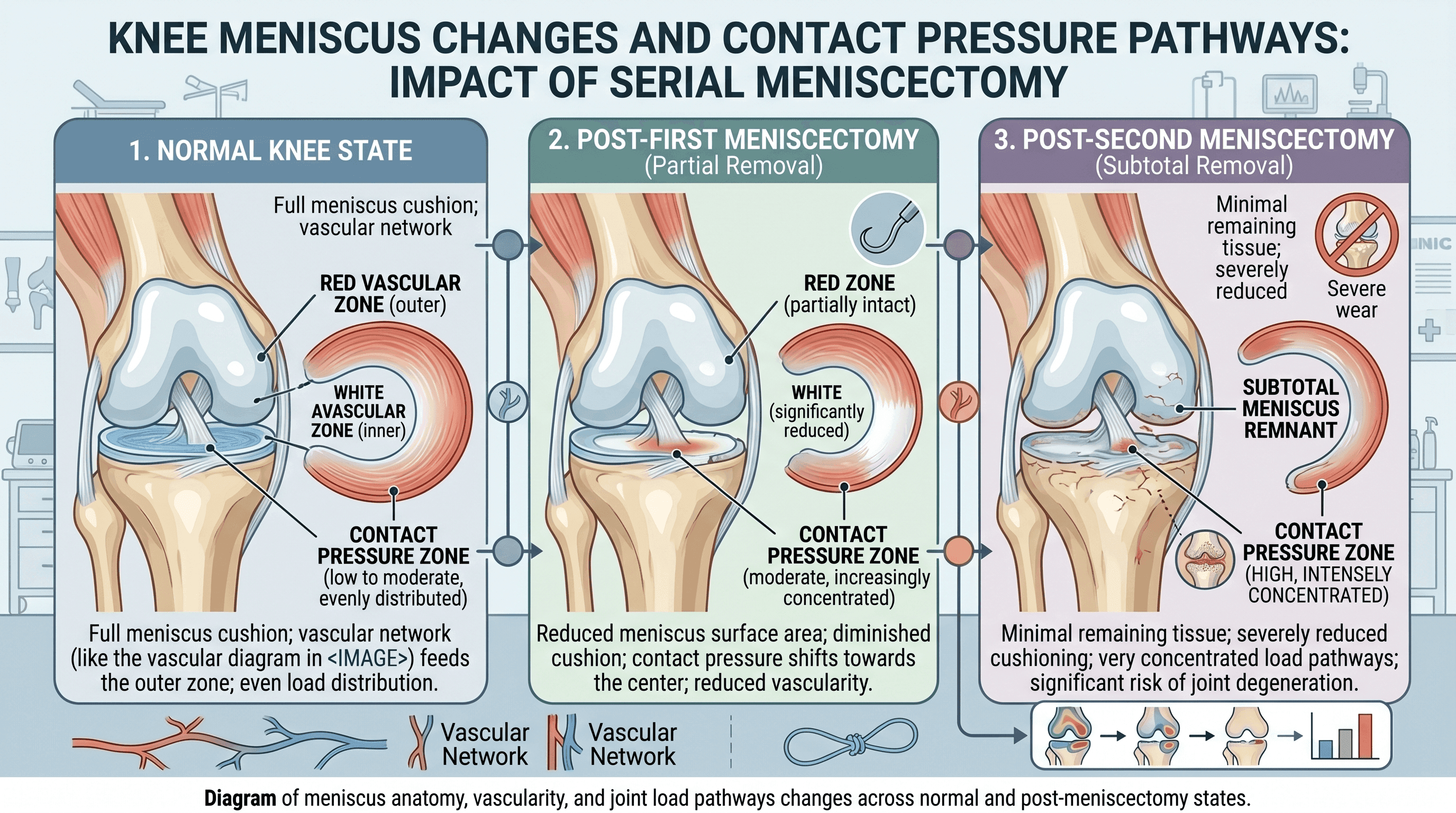
The practical implication is that a second meniscectomy may relieve short-term symptoms but accelerates the long-term thinning of joint cartilage. Surgeons performing a second trimming procedure typically aim to remove only the absolute minimum necessary to stabilize the joint, preserving every possible millimeter of healthy tissue.
Can a Failed Meniscus Repair Be Stitched Again?
This is one of the most common questions a returning patient asks, and the answer depends on tissue quality more than anything else.
Revision Repair: When the Tissue Is Still Worth Saving
If imaging and arthroscopic examination show that the remaining meniscal tissue is structurally viable, a second suture repair, called a revision repair, is technically possible. A 2021 meta-analysis via PMC found a long-term failure rate of approximately 19 percent for primary meniscus repairs, and revision repairs carry a higher failure risk than initial repairs. Despite this, revision repair remains preferable to trimming when the tissue can support it, because preserving meniscal volume protects the joint over decades.
Concurrent ACL reconstruction, when performed at the same time as a revision repair in patients with associated ligamentous instability, has been shown to improve healing outcomes. Ligament stability is a prerequisite for reliable meniscal healing.
Partial Meniscectomy: Faster Recovery, but an Irreversible Trade-Off
When the tissue is not viable for re-suturing, partial meniscectomy becomes the fallback. Recovery from a second partial meniscectomy is typically shorter than revision repair, often 6 to 12 weeks before return to light activity, but the trade-off is permanent. Removed meniscal tissue does not regenerate, and the consequences for joint health compound over time.
"Meniscal tissue is irreplaceable. Every effort should be made to preserve it before considering resection." Cleveland Clinic, Meniscus Repair Overview
The Biggest Risk of Multiple Surgeries: Accelerated Osteoarthritis
The most significant long-term consequence of repeated meniscus procedures is accelerated osteoarthritis. Each surgery, particularly each meniscectomy, leaves the knee with less cartilage to distribute mechanical load. Over time, this can lead to bone-on-bone contact, persistent pain, and functional limitation that no further arthroscopic surgery can address.
A 2024 review published via PMC confirmed that prior meniscal surgery is an independent risk factor for the development of knee osteoarthritis, with the risk increasing with the number of procedures performed. Younger patients who undergo multiple meniscectomies face the probability of developing clinically significant arthritis by their 40s or 50s.
This is not a reason to avoid necessary surgery. It is, however, a reason to take a long view when deciding between repair and removal, and a strong argument for pursuing every conservative option before committing to a third or fourth procedure.

Advanced Alternatives: Meniscal Allograft Transplantation
For patients who have lost too much meniscal tissue through prior surgeries to benefit from another repair or trimming procedure, meniscal allograft transplantation (MAT) is an option that deserves a serious conversation with an experienced knee surgeon.
MAT involves surgically implanting donor meniscal tissue from a cadaver to replace what has been removed. According to the American Academy of Orthopaedic Surgeons, ideal candidates for MAT are typically under 55 years of age, have no significant pre-existing osteoarthritis, have stable knee ligaments, and have a body weight within a healthy range for their frame.
A 2024 study published in the Knee Surgery and Sports Traumatology journal via Wiley found that MAT can produce meaningful improvements in pain and function for appropriately selected patients. Recovery from MAT is substantially longer than recovery from arthroscopic procedures, typically ranging from 6 to 12 months before return to unrestricted activity.
MAT does not reverse existing cartilage damage, but it can slow further deterioration and improve quality of life for patients who would otherwise face a direct path to joint replacement. It is a bridge procedure, not a cure, and its long-term durability depends heavily on the health of the remaining joint surfaces.
If you are considering MAT or want to understand whether you might be a candidate, find a knee specialist through Momentary Lab's physician directory to start that conversation.
When Is It Time to Skip the Arthroscopy and Consider Knee Replacement?
Not every patient returning with a painful knee after meniscus surgery is a candidate for another arthroscopic procedure. For some, particularly older patients with significant pre-existing joint degeneration, the honest conversation with a surgeon may be about partial or total knee replacement rather than a third attempt at cartilage repair.
Contraindications for Further Meniscal Surgery
Advanced osteoarthritis, significant malalignment of the knee joint, severe tissue degeneration, and obesity-related joint loading are all factors that reduce the likelihood that another meniscal procedure will provide lasting benefit. A 2019 article published via Springer noted that patient selection criteria for revision meniscal procedures require careful assessment of articular cartilage health, because even a technically successful repair cannot compensate for damaged joint surfaces.
When articular cartilage loss is severe and widespread, a partial or total knee replacement offers more predictable long-term pain relief and functional improvement than continued arthroscopic intervention. This is not a failure of the patient or the prior surgeons. It is a natural progression that some knee injuries eventually reach, particularly when the original injury was severe or occurred at a younger age, allowing decades of wear before joint replacement becomes appropriate.
The Counterintuitive Finding About Age
Younger age does not automatically confer better surgical outcomes for revision procedures. A review via PMC (2024) found that in certain cohorts, younger age was actually associated with higher revision failure rates, likely because younger patients tend to return to higher-demand activity levels that stress the healing tissue. This finding underscores why activity modification and realistic expectation-setting are as important as the surgical decision itself.
Recovery Round Two: Is the Rehab Harder the Second Time?
For most patients, yes, rehabilitation after a second meniscus surgery is more demanding than the first. The reasons are both biological and psychological.
Why Revision Repair Rehabilitation Is Slower Than You Expect
Scar tissue from the first surgery changes the tissue environment. Reduced vascularity in a previously operated joint, along with the lower mechanical quality of remaining meniscal tissue, means that healing after revision repair requires a more conservative loading progression than a primary repair. Surgeons typically extend weight-bearing restrictions and delay return-to-sport milestones by several weeks compared to first-time repair protocols.
According to protocols referenced by the American Academy of Orthopaedic Surgeons, patients undergoing revision meniscal repair should typically expect a minimum of 4 to 6 months of structured rehabilitation before return to pivoting or impact sport, and 6 to 9 months is more realistic for high-demand activities.
Biologic Augmentation: Can PRP or Fibrin Clot Improve Outcomes?
Platelet-rich plasma (PRP) and fibrin clot augmentation are emerging adjuncts to meniscal repair that aim to improve biological healing at the repair site. These techniques involve concentrating growth factors from the patient's own blood and applying them directly to the tear site during surgery.
The evidence base is still developing. Some studies have shown improved healing rates with biologic augmentation, particularly in white zone tears where blood supply is limited. This remains an active area of research and is worth raising with a surgeon as a specific discussion point, asking whether they routinely use augmentation for revision repairs and what the current evidence supports. It is not a standard of care universally adopted, but it represents a meaningful differentiator in how some centers approach revision surgery.

Questions to Ask Your Surgeon Before Agreeing to a Second Meniscus Operation
Walking into a surgical consultation without prepared questions is one of the most common ways patients leave feeling more confused than when they arrived. Use this list before any second-surgery decision is made.
Why did the first surgery fail? Ask the surgeon to explain specifically whether the failure was a new traumatic tear, failed biological healing, or a technical complication. The answer determines everything that follows.
Which type of second surgery are you recommending, and why? Make the surgeon walk through the choice between revision repair, meniscectomy, and MAT. Ask what makes the recommended option preferable for your specific anatomy and imaging findings.
How much meniscal tissue do I have left? Get a concrete answer in terms of percentage of the meniscus remaining. This sets the context for understanding long-term osteoarthritis risk and future options.
What is your experience with revision meniscal cases? Revision surgery is technically more demanding than primary repair. Surgeon volume and experience with revision cases matters. This is a fair and important question to ask directly.
What does my articular cartilage look like, and does it affect the recommendation? The condition of the surrounding joint cartilage is as important as the meniscus itself. If cartilage damage is already significant, a meniscal procedure may provide only temporary benefit.
What happens if this surgery also fails? Understanding the escalation pathway before committing to a procedure gives you a clearer picture of the full decision tree.
Are there conservative options worth trying before surgery? Physical therapy, activity modification, anti-inflammatory management, and in some cases, corticosteroid or hyaluronic acid injections may provide adequate symptom control depending on the severity and location of the problem.
What does my recovery look like, and what is the return-to-activity timeline for my specific situation? Generic recovery timelines are less useful than a surgeon's specific estimate based on your anatomy, tissue quality, and activity goals.
FAQ
Can I have meniscus surgery twice?
Yes. A second meniscus surgery on the same knee is medically feasible in most cases, though the type of procedure depends on how much healthy tissue remains, the condition of the articular cartilage, and what caused the first surgery to fail or the tear to recur. A thorough evaluation with updated MRI imaging is typically needed before proceeding.
Which recovery is harder, ACL or meniscus?
Both recoveries are demanding, but ACL reconstruction typically involves a longer overall return-to-sport timeline, often 9 to 12 months, compared to 3 to 6 months for a straightforward meniscal repair. That said, a revision meniscal repair or MAT procedure can rival ACL recovery in length and intensity, particularly when conservative rehabilitation protocols are required to protect compromised tissue. A doctor can advise on individual cases based on the specific procedures involved.
Why does my knee still hurt 2 years after meniscus surgery?
Persistent pain two years after meniscus surgery may reflect a number of conditions: a re-tear or failed healing at the original repair site, the development of early osteoarthritis due to reduced cartilage volume, scar tissue formation, or an unrelated structural problem such as patellar tracking issues or cartilage defects. An updated MRI and consultation with an orthopedic surgeon is the appropriate next step to identify the specific cause.
How do you know if your meniscus is torn again after surgery?
Symptoms of a recurrent meniscal tear often mirror the original injury: new or worsening joint-line pain, swelling that comes on within 24 to 48 hours of activity, and mechanical symptoms such as clicking, locking, or the sensation that the knee is giving way. These symptoms warrant an orthopedic evaluation rather than a wait-and-see approach, particularly if they appear following a specific activity or movement.
How much meniscus can safely be removed?
There is no universally agreed threshold, but research has established that removing more than 50 percent of the meniscal tissue substantially increases joint contact pressure and osteoarthritis risk. Surgeons generally aim to preserve as much healthy meniscal tissue as possible, and cases requiring extensive removal are often reconsidered for repair or transplant alternatives.
Is meniscal allograft transplantation covered by insurance?
Coverage varies significantly by insurer and plan. MAT is generally considered a covered procedure when medical necessity criteria are met, typically including documented meniscal deficiency, absence of significant osteoarthritis, and prior failure of conservative management. Using the Momentary Lab AI Healthcare Navigator to understand your coverage options and navigate care decisions can help before committing to a procedure.
References
- PMC (2024) — Revision Meniscal Surgery Outcomes Review — Cited for age as a predictor of revision failure and osteoarthritis risk after repeated meniscal procedures.
- PMC (2021) — Meniscus Repair Long-Term Failure Rate Meta-Analysis — Cited for the approximately 19 percent long-term failure rate of primary meniscus repair.
- Knee Surgery and Sports Traumatology, Arthroscopy (Wiley, 2024) — Cited for outcomes data on meniscal allograft transplantation.
- Springer, Knee Surgery and Related Research (2019) — Cited for patient selection criteria and articular cartilage assessment in revision meniscal surgery.
- PubMed (2011) — Meniscus Repair Failure Rate Systematic Review — Cited for failed healing as a distinct failure mode from traumatic re-tear.
- PubMed (1990) — Contact Pressure Changes After Meniscal Removal — Cited for joint contact pressure increases after partial meniscectomy.
- Cleveland Clinic — Meniscus Repair Overview — Cited for the pull quote on meniscal tissue preservation.
- Mayo Clinic — Meniscus Tear — Cited for meniscal vascularization and blood supply zones.



