
Your surgeon said six weeks. A friend on the recovery forum said they were back behind the wheel in two. Your physical therapist says it depends. So who is right?
The honest answer: all of them, and none of them. Most patients can drive somewhere between 2 and 12 weeks after rotator cuff repair, but your timeline hinges on which arm was operated on, what type of procedure you had, and whether you clear a short but non-negotiable readiness checklist first. This guide walks through the research, breaks down each variable, and gives you a practical week-by-week framework for getting safely back on the road.
At a Glance
| Topic | Key Facts |
|---|---|
| Typical driving window | 2 to 12 weeks post-surgery |
| Shortest reported timeline | 2 weeks (arthroscopic repair, non-dominant arm, per Badger et al. 2022) |
| Longest timeline | 10 to 12 weeks (open repair, dominant arm) |
| Absolute blockers | Sling still on; narcotic pain medication; pain limiting shoulder-check |
| Dominant arm adds | Approximately 2 to 4 additional weeks over non-dominant |
| Manual transmission adds | Approximately 1 to 2 additional weeks |
| Clearance authority | Your orthopedic surgeon or physical therapist |
The Short Answer: Typical Driving Timelines by Surgery Type
The expected return-to-driving window varies by the type of rotator cuff procedure performed. Here is how the numbers break down across the most common procedures:
| Procedure | Typical Return-to-Driving Timeline |
|---|---|
| Arthroscopic debridement only | 1 to 2 weeks |
| Arthroscopic repair, non-dominant arm | 2 to 4 weeks |
| Arthroscopic repair, dominant arm | 6 to 8 weeks |
| Open rotator cuff repair | 8 to 12 weeks |
| Massive rotator cuff tear repair | 10 to 12 weeks |
| Bicep tenodesis (combined procedure) | 6 to 10 weeks depending on arm |
These timelines assume the sling has been removed, narcotic pain medication has been stopped for at least 24 to 48 hours, and the surgeon has given a formal green light. If any of those conditions are not met, the timeline does not apply.
Why Surgeons Give Such Different Answers
Until recently, no universal evidence-based guideline existed for driving after rotator cuff repair. Surgeons were working from clinical intuition rather than objective data, which explains the wide variation in advice patients receive.
That changed with the Badger et al. 2022 study, published in the Journal of Bone and Joint Surgery. The study enrolled 32 patients and used on-road instrumented vehicle assessment, which is an objective measure of real-world driving performance rather than a simulator. The researchers found that driving performance after arthroscopic rotator cuff repair was non-inferior to pre-surgical baseline as early as two weeks postoperatively. "Non-inferior" in this context means statistically indistinguishable from the patient's own pre-surgery driving ability, not merely "good enough." That is a meaningful standard.
A 2025 study published in the Journal of Experimental Orthopaedics surveyed return-to-driving patterns in a larger cohort. It found that 23% of patients had resumed driving at one month post-repair, 70% by two months, and 99% by six months. The wide spread reflects how much surgery type, arm dominance, and individual recovery pace influence the real-world timeline.
The takeaway: two weeks is biologically possible for some patients, but it is not a universal threshold. The research offers a floor for the best-case scenario, not a target for everyone.
The Absolute Dealbreakers: Narcotics and the Sling
Before any timeline discussion matters, two conditions must be resolved entirely. These are not gray areas.
The sling must be off, permanently. Operating a vehicle with a shoulder immobilizer in place is a safety hazard. The sling restricts the range of motion needed to turn the wheel, reach the gear selector, and perform emergency steering corrections. Beyond the physical limitation, most auto insurance policies require the driver to be in a physically fit condition to operate the vehicle. Driving in a sling after explicit medical instruction to wear one could expose the driver to liability in the event of an accident.
Standard sling wear after arthroscopic rotator cuff repair runs four to six weeks for the operated arm. Open repairs or massive tear repairs may require six to eight weeks of immobilization. So even in the best-case research scenario, the two-week return-to-driving result was achieved in patients who had already been cleared to remove their sling. If the sling is still on, the two-week timeline is simply not applicable to that patient.
Narcotic pain medication must be stopped. Opioid analgesics prescribed after rotator cuff surgery, including oxycodone, hydrocodone, and tramadol, impair reaction time, depth perception, and cognitive processing speed. Driving while taking narcotics constitutes impaired driving under the laws of every US state, regardless of whether the medication was legally prescribed. Beyond the legal exposure, the physical risk is real: a study published in Clinical Orthopaedics and Related Research found that opioid-impaired reaction time increases significantly enough to affect emergency braking performance. Most surgeons recommend being off narcotics for a minimum of 24 to 48 hours before attempting to drive. If over-the-counter pain relievers are not controlling the pain adequately at that point, the shoulder is probably not ready for driving demands anyway.
Right Arm vs. Left Arm: Does It Change the Timeline?
This is one of the most underappreciated variables in rotator cuff recovery, and most patients do not hear about it until they are already frustrated with a slower-than-expected return.
The short answer: yes, it changes the timeline significantly.
Why Dominant Arm Surgery Takes Longer
The dominant arm carries a disproportionate share of steering demand. Upper steering wheel placement, which is the natural grip position most drivers use, activates the rotator cuff substantially more than lower-wheel contact. EMG research cited in the Badger et al. 2022 study confirmed that muscle activation patterns during steering load the repaired tissue in ways that can stress suture anchors in the early healing phase.
Beyond routine steering, the dominant arm is the primary driver for emergency maneuvers, sharp cornering, and hand-over-hand turning. These are not everyday actions, but they are the exact demands that an accident scenario would place on a newly repaired rotator cuff.
A simulator study by Jazrawi and colleagues found that collision rates nearly doubled at six weeks post-surgery for dominant-arm patients compared to pre-operative baselines. By twelve weeks, collision rates had returned to normal. That twelve-week window for dominant-arm patients aligns with the conservative end of surgical guidance and reflects a real protective reason for the extended restriction.
Non-Dominant Arm Recovery
Non-dominant arm patients have a meaningfully different profile. The non-dominant arm handles lower steering wheel contact, signaling, and minor corrections rather than primary steering force. The Badger et al. 2022 study's two-week return-to-driving finding was most applicable to this group: arthroscopic repair of the non-dominant arm with an otherwise uncomplicated recovery.
Practically, non-dominant arm patients cleared by their surgeon can often return to driving at four to six weeks post-surgery, sometimes earlier if the readiness checklist is fully met.
Manual Transmission Adds Time for Both Groups
Manual transmission demands bilateral shoulder engagement: left hand on the wheel while the right shifts, followed by left-hand-only steering during the shift, combined with clutch pedal pressure that transfers to the torso and shoulder. Research cited in the orthopaedic literature indicates that patients driving manual vehicles should add approximately one to two weeks to their estimated timeline, regardless of which arm was operated on. If manual driving is unavoidable, keeping both hands on the lower half of the steering wheel reduces rotator cuff activation meaningfully compared to upper-wheel grip.
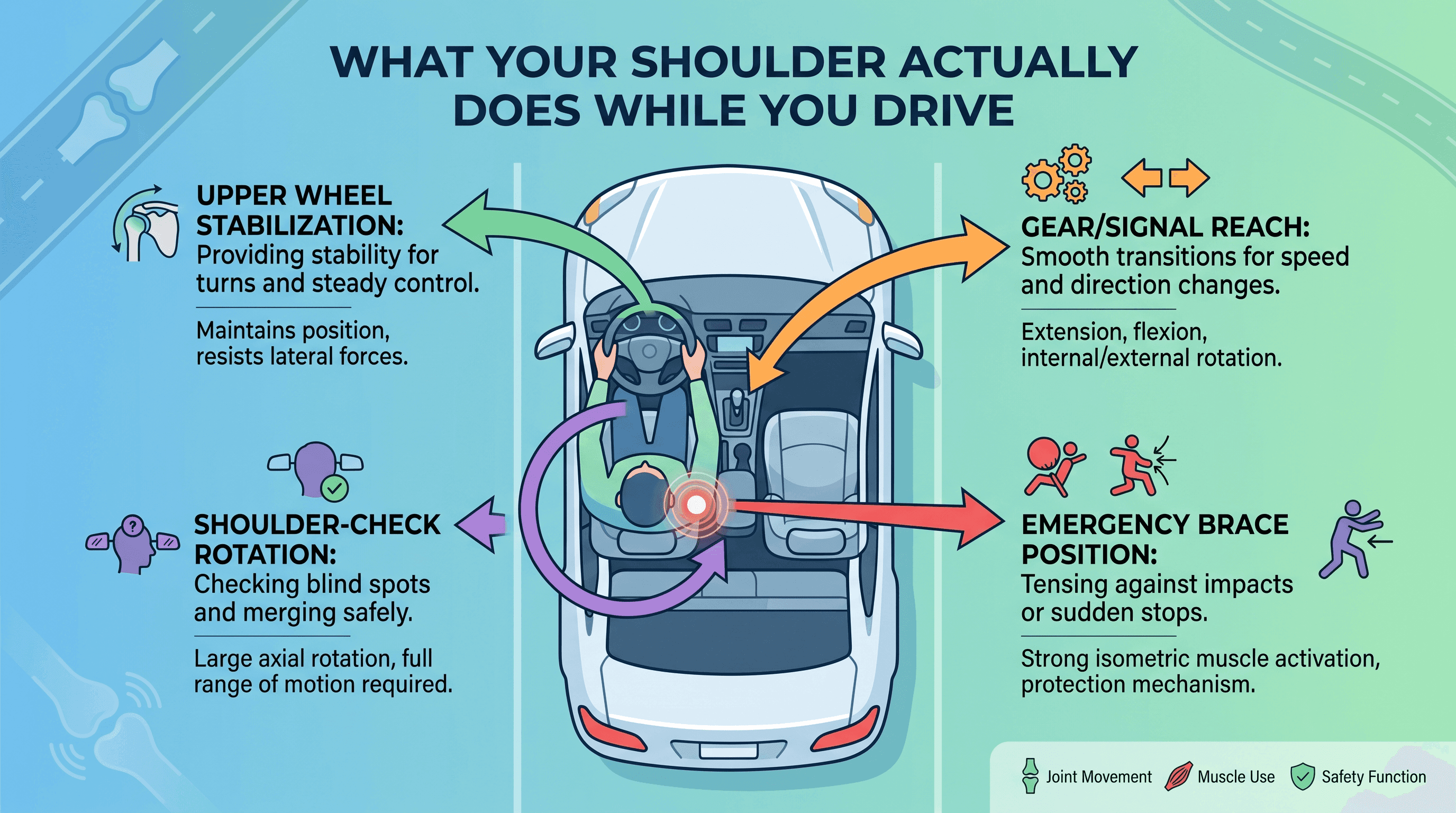
The Hidden Physical Demands of Driving
Driving feels passive, but the shoulder does more work than most patients anticipate during recovery.
Routine driving involves continuous low-level isometric stabilization of the shoulder girdle to hold the wheel, manage vibration, and track the road. More demanding is the emergency braking scenario: a sudden hard stop requires simultaneous upper extremity bracing and wheel control. In this situation, the forces transmitted through the shoulder can exceed what the healing repair is able to handle in the first several weeks.
Turn signals, reversing, and parking maneuvers require shoulder external rotation and extension. Shoulder-checking for lane changes specifically demands cervical rotation combined with shoulder movement, which can be painful and distracting long after the acute surgical pain resolves. Any hesitation in a shoulder-check during active traffic is a meaningful safety risk.
The clinical implication is straightforward. Patients who cannot perform a shoulder-check without pain or hesitation, even at four or six weeks post-surgery, are not ready to drive regardless of what the calendar says.
The Seatbelt Problem: Comfort and Safety
The standard three-point seatbelt crosses directly over the surgical shoulder on the driver's side. For patients who had surgery on the right shoulder, a normally worn seatbelt applies pressure directly to the repaired cuff and the incision site on every bump, deceleration, and turn. For left-shoulder patients driving standard US vehicles, the belt rides on the non-operated side, which is considerably less of an issue.
Right-shoulder patients often find the seatbelt uncomfortable enough in early recovery to adjust how they wear it, which creates a legitimate safety problem. Wearing the belt incorrectly to avoid pressure on the shoulder significantly reduces its effectiveness in a collision. Padded seatbelt covers designed to cushion the strap over the shoulder can reduce pressure without compromising belt position. These are widely available and serve a real purpose for this population, but they do not replace medical clearance for driving.
One practical strategy: place a small pillow or rolled towel between the seatbelt and the shoulder during short recovery drives. This reduces direct pressure while keeping the belt in its correct position. Always verify the seatbelt remains snugly positioned across the chest and pelvis regardless of what padding is used.
The 5-Point Self-Readiness Checklist Before You Drive
This checklist applies once a surgeon or physical therapist has confirmed the sling can be removed and narcotic medications have been stopped. All five points must be satisfied before attempting to drive.
The following checklist reflects the functional criteria referenced in the Badger et al. 2022 research protocol and standard orthopedic clinical guidance.
Check 1: The sling has been removed permanently for at least 24 to 48 hours. Not just taken off for meals or physical therapy. Permanently off, per surgeon instruction.
Check 2: No narcotic or sedating pain medication for at least 24 to 48 hours. This includes oxycodone, hydrocodone, tramadol, gabapentin (at sedating doses), and prescription muscle relaxants. Over-the-counter NSAIDs such as ibuprofen and acetaminophen are generally acceptable, but confirm with the prescribing physician.
Check 3: Both arms can be raised to at least shoulder height without significant pain. If raising the operated arm to shoulder height produces sharp, stopping pain, emergency steering will be beyond reach.
Check 4: The steering wheel can be gripped and rotated through a full left-to-right range without hesitation. The best way to test this: sit in a parked, stationary car and physically turn the wheel from lock to lock. If this produces pain, guarding, or weakness at any point, do not drive.
Check 5: A shoulder-check can be performed comfortably in both directions. Full-speed active traffic requires an unimpeded, instinctive shoulder-check. If the motion is delayed, painful, or requires conscious effort, reaction time in traffic will be compromised.
Testing items 3 through 5 in a parked, stationary vehicle before the first actual drive is strongly recommended. This takes less than two minutes and avoids discovering a limitation in motion while already on the road.
The Official Clearance: Who Makes the Call?
Surgical clearance to drive is not automatic at any time point. It is a formal decision made by the orthopedic surgeon or, in many cases, the physical therapist managing the post-operative rehabilitation program.
The reason clearance matters beyond just personal judgment is liability. If a patient is involved in a motor vehicle accident while recovering from shoulder surgery and has not been formally cleared to drive, auto insurance carriers in many states can investigate whether the driver was medically fit to operate a vehicle. Policies often include clauses requiring the insured to be physically capable of safe vehicle operation. A notation in the medical record that driving was not yet cleared could constitute grounds for claim denial. Patients should ask their surgeon or PT to document the driving clearance decision in writing.
Clearance is also not permanent. If a patient experiences a sudden setback such as a fall on the operated arm, a new onset of weakness, or a suspected repair failure, driving restrictions may be re-imposed. Any new acute pain or mechanical symptom after a period of improvement should prompt contact with the surgical team before continuing to drive.
If an earlier return to driving is medically necessary, such as for sole caregivers or individuals with transportation-dependent work, that conversation belongs with the surgeon. Some practices have access to occupational therapists who perform formal behind-the-wheel assessments for post-surgical patients. This is a legitimate pathway and worth asking about if the standard timeline creates genuine hardship.
To find an orthopedic specialist or connect with a physician who can formally evaluate driving readiness after shoulder surgery, search for a qualified doctor near you.
Tips for Easing Back Onto the Road After Clearance
The goal of the first few post-clearance drives is not to prove the shoulder works. It is to rebuild confidence and identify any remaining limitations in a low-risk environment before returning to full driving demands.
Start with a five to ten minute drive in a low-traffic area, ideally in daylight, on familiar roads, and with another adult in the vehicle. Parking lots during off-peak hours are an excellent first environment. Avoid highway on-ramps, freeway merging, and heavy urban traffic for the first week back.
Keep both hands on the lower half of the steering wheel during early recovery drives. Lower wheel placement activates the rotator cuff muscles less than the ten-and-two position, per EMG research on steering biomechanics. This is a simple, evidence-informed adjustment that reduces load on the healing repair.
Set mirrors, adjust the seat, and position the seatbelt before starting the engine each time. Twisting and reaching after the engine is running introduces unexpected shoulder loading before the mind is focused on driving.
Gradually increase drive duration and complexity over two to three weeks. A reasonable progression: parking lot practice on day one, short neighborhood drives in week one, suburban roads and light traffic in week two, highway driving by week three if all prior steps went smoothly.
When to Call Your Surgeon Before Getting Behind the Wheel
Certain symptoms are not part of routine rotator cuff recovery and should pause any driving plans until evaluated by the surgical team.
Pain that persists well beyond the expected recovery window, especially pain that is not improving week over week, may indicate the repair has not healed as anticipated. Sudden new weakness in the operated arm, particularly the inability to raise the arm that was possible days before, warrants prompt orthopedic evaluation. A popping or clicking sensation accompanied by pain is different from the painless mechanical sounds common during early recovery and should be reported.
Patients who are uncertain whether their current pain level or medication regimen allows for safe driving should not self-authorize. A brief call or portal message to the surgical team can clarify this quickly.
Sole caregivers with urgent transportation needs should ask specifically about adaptive strategies, earlier physical therapy milestones, or occupational therapy driving evaluation as alternatives to waiting the full conservative timeline.
For personalized guidance on navigating your recovery and finding the right care, explore health information and care options here.
Frequently Asked Questions
Can I drive 2 weeks after rotator cuff surgery?
For a small group of patients, yes. The Badger et al. 2022 study found that driving performance after arthroscopic rotator cuff repair was non-inferior to pre-surgical baseline at two weeks in 32 patients assessed with on-road instrumented testing. However, this finding applies most directly to non-dominant arm repairs, patients already cleared to remove their sling, and those who have been off narcotic pain medication for at least 24 to 48 hours. Dominant arm repairs, open procedures, and massive tear repairs generally require considerably longer. Two weeks is a best-case floor based on current research, not a universal target.
What is the 7-minute rotator cuff solution?
The "7-minute rotator cuff solution" is a popular phrase used to describe short daily exercise routines promoted for shoulder health and rotator cuff strengthening. It is not a surgical or medical protocol. If a physical therapist has recommended a specific home exercise program for your post-operative rehabilitation, follow that protocol rather than general internet programs, as exercises appropriate for an intact shoulder may not be safe for a recently repaired one. A doctor can advise on individual cases.
Can I sleep without my sling 4 weeks after rotator cuff surgery?
This depends on the specific surgical repair and individual healing progress. Many arthroscopic repair patients are allowed to sleep without the sling at four to six weeks if the surgeon approves, particularly if daytime sling use is transitioning to weaning. Some patients find sleeping with a pillow under the operated arm provides support and comfort during this period. The decision should always be confirmed with the orthopedic surgeon managing the case, as removing the sling too early during sleep can result in unintended stress on the repair, particularly if the arm drops into extension during deep sleep.
Does driving aggravate the rotator cuff?
Yes, driving can aggravate a recovering rotator cuff if done before the tissue has healed sufficiently. Routine driving requires continuous isometric stabilization of the shoulder. Emergency braking, sharp turns, and upper-wheel steering all place sudden loads on the repaired tissue. Even seat vibration transmits to the shoulder girdle over longer drives. This is precisely why driving restrictions exist after rotator cuff repair, and why the readiness checklist matters rather than relying on a calendar date alone.
Do bicep tenodesis patients have different driving restrictions?
Bicep tenodesis, which is often performed alongside rotator cuff repair to address a damaged bicep tendon, adds additional healing considerations. The repaired bicep tendon is stressed by resisted forearm supination, gripping, and elbow flexion under load, all of which occur during driving. Most orthopedic surgeons apply driving restrictions similar to or slightly longer than the rotator cuff repair guidelines for combined procedures. Patients with a bicep tenodesis should confirm their specific driving timeline directly with their surgeon rather than applying standard rotator cuff timelines alone.
References
-
Badger SA et al. "Patients Who Undergo Rotator Cuff Repair Can Safely Return to Driving at 2 Weeks Postoperatively." J Bone Joint Surg Am. 2022. — Primary study demonstrating non-inferior on-road driving performance at 2 weeks post arthroscopic rotator cuff repair.
-
Antoni M et al. "Return to Driving After Rotator Cuff Repair." Journal of Experimental Orthopaedics. 2025. — Cohort data showing 23% return at 1 month, 70% at 2 months, 99% by 6 months post-repair.
-
Schuster P et al. "Return to Driving After Orthopaedic Surgery." PubMed. 2022. — Research on bilateral shoulder engagement demands in manual and automatic vehicle operation.
-
Verma NN et al. Study on opioid use and driving reaction time after orthopedic procedures. Clin Orthop Relat Res. 2015. — Cited for opioid effects on reaction time and emergency braking performance.
-
Olson M et al. Driving after rotator cuff surgery: simulator and on-road study data. PubMed. 2022. — Referenced for dominant vs. non-dominant arm driving outcomes and simulator collision rate data.



