
At a Glance
| Topic | Key Facts |
|---|---|
| Primary keyword | How long does rotator cuff surgery take to heal |
| Average full recovery | 6 to 12 months depending on tear size |
| Sling phase | 4 to 6 weeks (sometimes up to 8 weeks for large tears) |
| Return to desk work | 1 to 2 weeks post-op |
| Return to heavy labor or sports | 6 to 12 months |
| Tendon-to-bone fusion window | 8 to 12 weeks |
| Re-tear risk | 15 to 21% overall; higher for massive tears |
| Maximum Medical Improvement (MMI) | Typically reached at 12 months |
The Short Answer: The 6 to 12-Month Marathon
Most people expect to feel functional within a few weeks of rotator cuff surgery. That expectation needs recalibrating before the operation even happens.
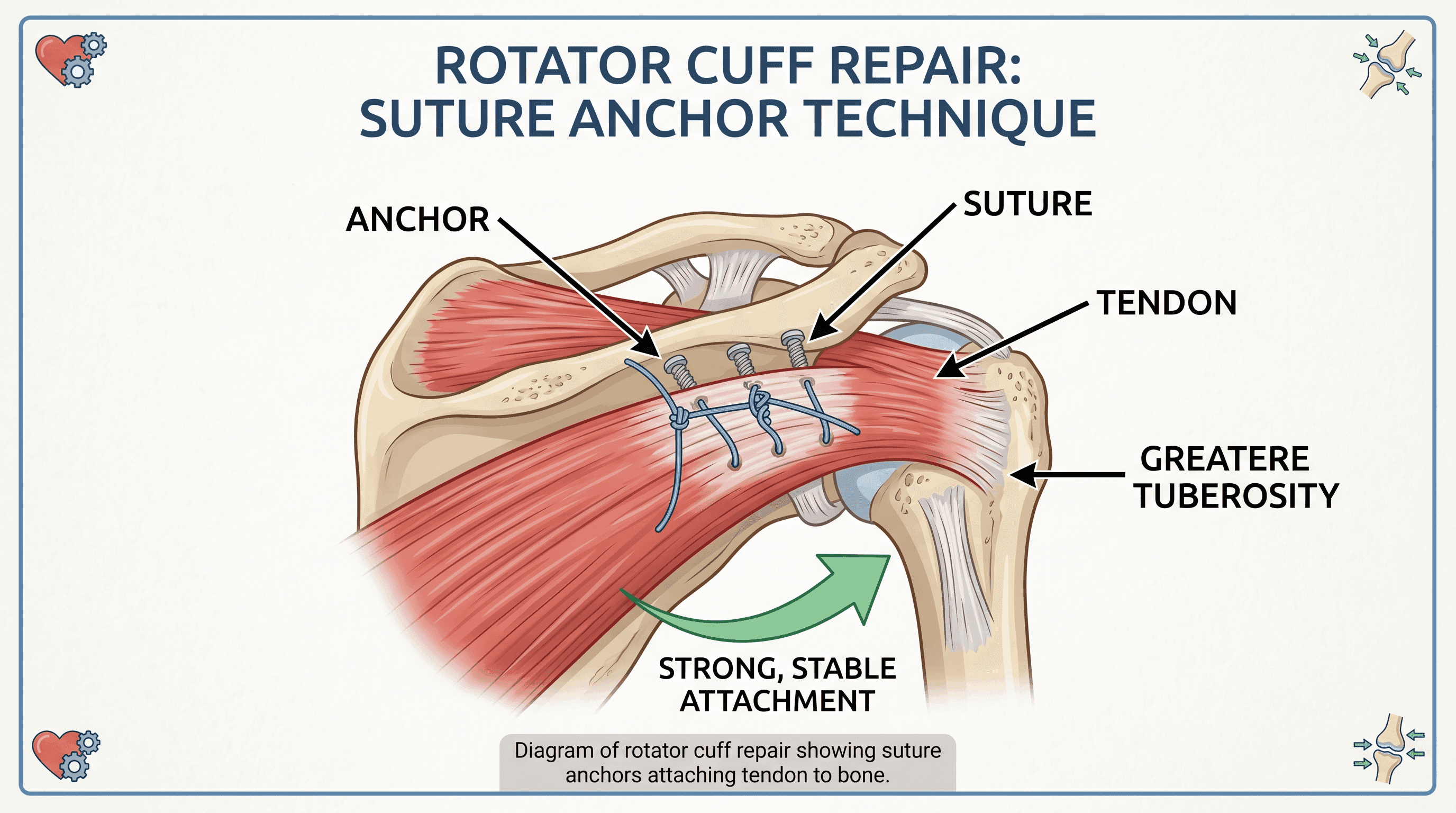
The rotator cuff is a group of four tendons that wrap around the head of the upper arm bone and keep the shoulder stable during every lift, reach, and rotation you make. When a surgeon repairs a torn rotator cuff, the goal is to reattach the tendon directly to bone using small titanium or absorbable anchors threaded with sutures. That reattachment is not instant healing. It triggers a biological process that takes months to complete, and the shoulder does not know how impatient you are.
Here is a quick reference table before going deeper into each phase:
| Tear Size | Approximate Full Recovery |
|---|---|
| Small (less than 1 cm) | 4 to 5 months |
| Medium (1 to 3 cm) | 4 to 6 months |
| Large (3 to 5 cm) | 6 to 9 months |
| Massive (greater than 5 cm) | 9 to 12 months or longer |
These ranges reflect functional recovery, meaning the shoulder is strong enough to tolerate normal daily life and most recreational activities. Biological maturation of the repaired tendon takes longer, often up to a full year.
What "Healed" Actually Means
There are three distinct milestones on the road to a healed rotator cuff, and they are not the same thing.
The first milestone is initial tendon-to-bone contact, which the surgeon achieves in the operating room. The anchors hold the tendon in place, but the tissue is not yet fused. At this stage, the repair is held entirely by sutures and anchors, not by living tissue.
The second milestone is structural integrity, typically reached between 8 and 12 weeks. This is when scar tissue has matured enough to contribute real mechanical strength to the repair. According to research published by the National Institutes of Health, this biological consolidation phase controls the pace of early rehabilitation more than any other factor. Pushing through this window with heavy resistance exercise is the leading cause of re-tears.
The third milestone is functional strength recovery, which takes 6 to 12 months depending on tear size, age, and adherence to physical therapy. Some patients, particularly overhead athletes and manual workers, describe the shoulder as "not quite right" for the first nine months even when imaging shows a successful repair. According to Johns Hopkins Medicine, full strength is generally not recovered until approximately nine months post-surgery. That timeline is normal and expected.
Why Healing Takes So Long: The Biology Explained
Understanding why rotator cuff surgery recovery is measured in months rather than weeks starts with understanding what the surgery actually does.
When a surgeon repairs a rotator cuff arthroscopically, the first task is to freshen the bone surface where the tendon originally attached. The surgeon uses a small burr to create a bleeding surface on the greater tuberosity, the bony prominence of the upper arm, because living bone stimulates tendon regrowth better than smooth, worn bone. Suture anchors, typically 4 to 6 millimeters wide, are then drilled into the bone and loaded with high-strength sutures. Those sutures are threaded through the torn tendon and pulled down so the tendon lies flat against the prepared bone surface.
The result is not a healed tendon. It is an engineered biological attachment waiting to grow. The tendon and bone must form a new fibrovascular interface, which progresses through three overlapping phases: an inflammatory phase in the first two weeks where blood vessels grow into the repair, a proliferative phase from weeks 2 through 8 where collagen is laid down, and a remodeling phase from 8 weeks to 12 months where that collagen matures and aligns under mechanical load. Each phase must complete before the next can reach full effect.
The reason this differs from, say, a skin laceration healing in 10 days is blood supply. Skin is richly vascularized. Tendon tissue, particularly at the attachment site, has one of the poorest blood supplies in the body. Research published in PMC confirms that the hypovascular nature of tendon-bone junctions is the primary biological reason for extended recovery timelines after rotator cuff repair.
That is also why smoking, diabetes, and age have such an outsized impact on outcomes. Each condition compromises the vascular and cellular machinery that powers this slow, methodical process.
Week-by-Week Rotator Cuff Recovery Timeline
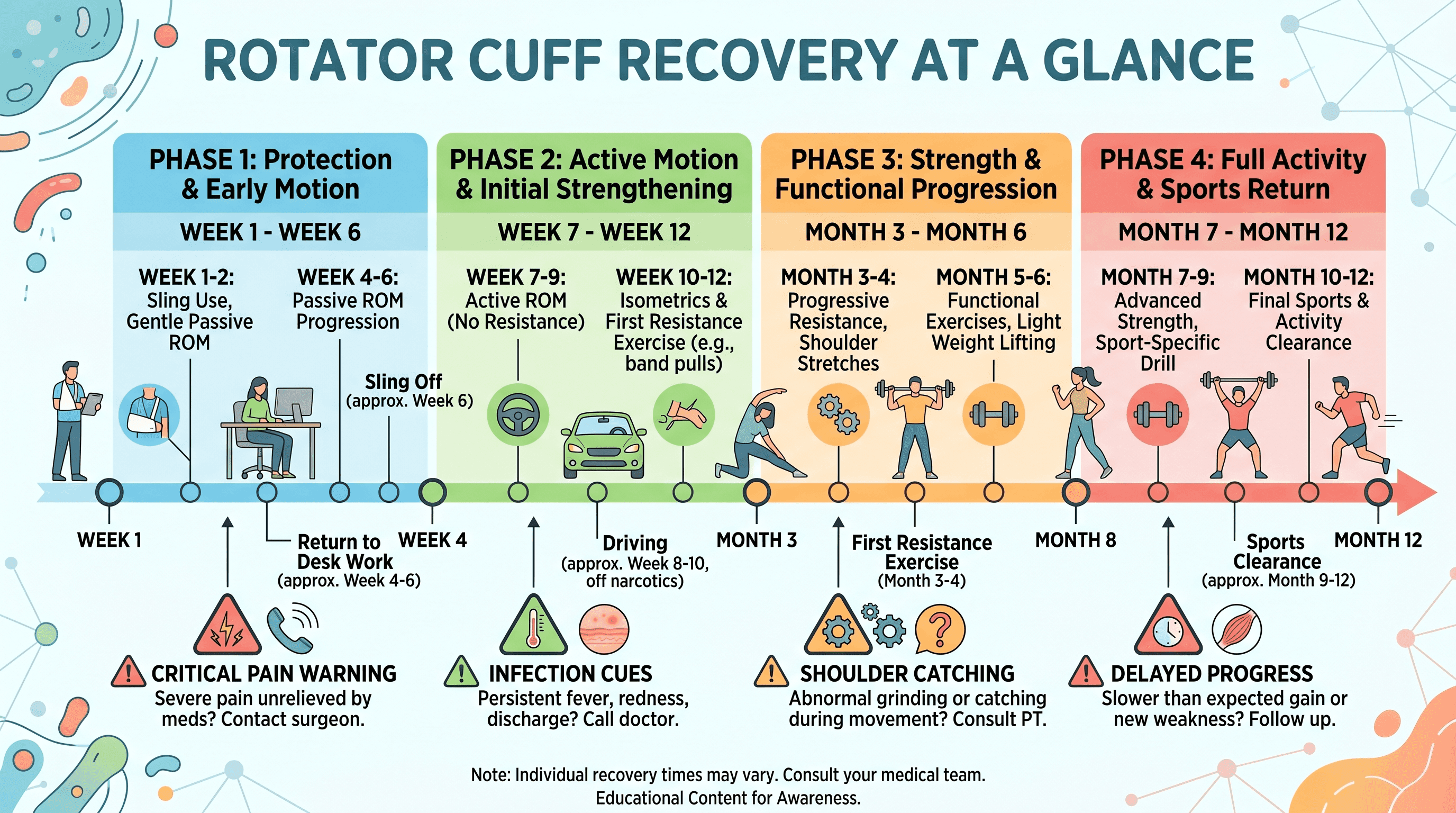
Recovery from rotator cuff surgery moves through five distinct phases. The phases are not rigid calendar events. They are biological thresholds, and a surgeon's clearance, not the date on a calendar, marks the passage from one to the next.
Weeks 1 to 2: Protection Phase
The first two weeks after surgery are about protection above everything else.
The repair is held by sutures and anchors only. No meaningful tendon-to-bone fusion has occurred yet, and the repair can fail if the shoulder is loaded incorrectly. The arm rests in a sling 24 hours a day, including during sleep. The only sanctioned shoulder movement at this stage is pendulum exercises, where the patient leans forward and lets the arm swing gently under gravity with no active muscle contraction. The movement keeps the joint fluid circulating and prevents the worst of early stiffness without stressing the repair.
Icing the shoulder for 20 minutes every one to two hours is standard for the first 72 hours and remains useful for reducing swelling through the first two weeks. Pain management typically involves a short course of prescription pain medication, transitioning to over-the-counter anti-inflammatory medication as comfort allows. A surgeon will provide specific wound care instructions, usually keeping the incision sites dry for the first 48 to 72 hours.
The most overlooked part of this phase is preparing the home environment before surgery, not after. A recliner chair or a large wedge pillow positioned at 30 to 45 degrees is far more comfortable than a flat bed for the first two weeks. Meals, childcare, transportation, and tasks requiring two hands should be arranged in advance. One-arm dressing tips (button-front shirts, slip-on shoes, loose waistbands) save significant frustration once the sling is on.
Weeks 3 to 6: Early Passive Motion Phase
The focus shifts in weeks 3 through 6 from pure protection to controlled movement, but the operative word is passive.
Passive range of motion means a physical therapist or the patient's own other hand moves the surgical arm through its range. The rotator cuff muscles themselves remain disengaged. This distinction matters because active muscle contraction loads the repair before the tendon has developed enough structural strength to tolerate it safely.
Physical therapy typically begins around week 2 to 3 with passive forward elevation and external rotation. The sling begins to be weaned around week 4 for most patients with small to medium tears. Larger tears often require 6 to 8 weeks of full-time sling use, and a surgeon's guidance takes precedence over general timelines.
Driving clearance for the non-dominant arm typically comes between 2 and 4 weeks for automatic transmission vehicles, provided the patient is off narcotic pain medication and able to grip the steering wheel confidently. Dominant-arm driving generally waits until 4 to 6 weeks.
Sleep comfort improves meaningfully between weeks 4 and 6 for most patients. Before that, a recliner or the 30 to 45-degree wedge pillow position reduces pressure on the shoulder joint compared to lying flat, where the surgical arm tends to fall forward and internally rotate painfully during sleep.
Weeks 7 to 12: Active Motion Phase
The transition to active motion is a significant milestone, but it is not permission to push through discomfort.
Active motion means the patient begins using their own shoulder muscles to move the arm, starting with gravity-eliminated positions and progressing to full elevation. Stiffness is the primary adversary during this phase, particularly for patients who develop adhesive capsulitis, a freezing of the joint capsule from prolonged immobilization. Consistent attendance at physical therapy and diligent home exercise program completion directly determines range of motion outcomes.
By week 12, the repair has developed sufficient biological strength to begin tolerating resisted exercise. This is when physical therapy introduces light resistance bands, progressing very gradually. Desk work and light daily activities like cooking and personal care are generally back to normal for most patients by this point.
"Healing of the rotator cuff tendon to bone is a complex biological process and takes months to achieve adequate strength for rehabilitation activities to be progressed." NIH / PMC, Rotator Cuff Repair Biology
The temptation to skip the week 12 threshold is the single most common cause of re-tears. Patients who feel good at 8 weeks and resume overhead activities or gym work before the biology supports it are not making up time; they are risking the entire repair.
Months 4 to 6: Strengthening Phase
The strengthening phase is where recovery starts to feel like progress patients can see and measure.
Resistance bands give way to light free weights. Physical therapists introduce rotator cuff-specific exercises, shoulder blade stabilization work, and progressive loading of the repaired tendon. By month 4 to 5, most patients can perform activities of daily living comfortably, sleep on their back, and carry grocery bags with the surgical arm.
Return to work timelines vary significantly by job type. Desk jobs and remote work are generally possible within 1 to 2 weeks of surgery, provided the sling is worn and no bilateral keyboard work is required. Light physical work, including jobs requiring occasional carrying of objects under 10 pounds, typically clears around 3 to 4 months. Overhead work and heavy manual labor, including construction, warehousing, and agricultural work, waits until 5 to 6 months at minimum, and often longer for large tears.
Non-contact recreational sports like cycling, walking, and stationary rowing typically clear around the 4 to 5-month mark. Contact sports and overhead sports wait for a later phase.
Months 6 to 12: Return to Full Activity
The final phase of recovery is the longest and often the most psychologically challenging, because the shoulder may feel mostly functional but surgical clearance for full activity has not yet arrived.
Cleveland Clinic notes that return-to-sport timelines for arthroscopic rotator cuff repair vary based on the demands of the activity. Non-contact sports are generally cleared around 6 months. Golf, swimming, and overhead racket sports typically require 9 months. Contact sports and overhead athletes, including baseball pitchers, competitive swimmers, and volleyball players, may wait up to 12 months before full return.
Heavy manual labor involving repetitive overhead lifting commonly gets the green light between 9 and 12 months. Patients should expect to have a formal conversation with their surgeon at the 9-month mark if they have not been formally cleared for their target activity.
It is normal for the shoulder to ache after prolonged activity at the 6-month mark. That is not a sign that something is wrong. The tendon is still remodeling and responding to load, and the muscles are still building back endurance after months of protective weakness. The ache that follows a long day of work or a round of golf typically diminishes over the following months as the repair matures.
The 1-Year Mark: Maximum Medical Improvement (MMI)
Maximum Medical Improvement is the point at which a patient's condition has stabilized and is unlikely to improve further with continued treatment.
For rotator cuff repair, MMI is typically declared at 12 months post-surgery. Most patients reach a functional plateau between 9 and 12 months, and the difference between those two endpoints is usually subtle. A small percentage of patients, particularly those with massive tears, multiple tendon involvement, or pre-existing fatty infiltration of the muscle, may retain a permanent 5 to 10% deficit in overhead strength or endurance compared to the unaffected shoulder.
What does "fully healed" actually mean at the one-year mark? For most patients, it means the repaired tendon has reached its maximum biological maturity. The collagen structure has remodeled under load, the scar tissue has softened and lengthened, and the rotator cuff muscles have regained close to their pre-injury strength. Some patients describe occasional weather-related aches or awareness of the shoulder in specific positions. That is not failure. It is a normal long-term outcome of tendon repair and consistent with data from PubMed-indexed studies on rotator cuff outcomes.
For workers' compensation and disability determinations, MMI carries legal weight, and a treating physician documents it formally. Patients who are still in recovery or anticipating a return to demanding physical work should ensure their surgeon has clearly defined the MMI date and functional capacity in writing.
What Slows Down the Healing Process?
Recovery timelines from rotator cuff surgery are not fixed. Several factors can meaningfully extend them, and understanding which ones are within a patient's control and which are not helps set realistic expectations without assigning blame.
Factors You Can Control
Smoking is the most significant modifiable factor affecting tendon-to-bone healing. Nicotine causes vasoconstriction, reducing blood flow to the repair site and starving the healing tissue of oxygen and nutrients. A 2024 study published in Cureus found that smokers had significantly higher rates of rotator cuff repair failure compared to non-smokers. Cessation before surgery improves outcomes; cessation during recovery, while harder to measure, is still recommended.
Blood glucose control matters because elevated glucose impairs both wound healing and the collagen-forming cells responsible for tendon repair. Patients with poorly controlled diabetes face a slower recovery curve and higher infection risk at incision sites. Working with a primary care physician to optimize A1c levels before and after surgery gives the repair the best biological environment.
Protein intake is an underappreciated lever. Tendon repair is a protein-synthesis-intensive process. Patients who consume adequate protein (generally 1.2 to 1.6 grams per kilogram of body weight daily) during the proliferative and remodeling phases provide the raw materials their body needs to build new collagen. A registered dietitian can advise on individual targets.
Physical therapy adherence is the single most impactful modifiable factor across all published rotator cuff recovery literature. Missing sessions, skipping home exercises, or stopping PT early because the shoulder "feels fine" consistently correlates with inferior functional outcomes at 12 months.
Sleep quality influences tissue repair more than most patients realize. Growth hormone secretion, which plays a direct role in musculoskeletal recovery, is highest during deep sleep. Prioritizing sleep architecture during recovery is not optional.
Factors Outside Your Control
Age is the strongest predictor of rotator cuff healing outcomes. Tendon quality, blood supply, and cellular repair capacity all decline with age, and this is not reversible. A 2025 umbrella review of rotator cuff repair outcomes confirmed that patients over 65 have measurably lower healing rates and higher re-tear risk than younger patients. This does not mean surgery is not worth pursuing; it means expectations for timeline and maximum strength recovery need to be calibrated accordingly.
Tear size and tissue quality are established at the time of injury, not at the time of surgery. A massive tear with retracted, degenerated tendon tissue presents a fundamentally different repair challenge than a fresh, small acute tear with supple tissue. Surgeons assess tissue quality intraoperatively, and some tears require augmentation with patches or alternative repair techniques.
Chronicity of the tear matters because a tendon that has been torn for months or years undergoes fatty infiltration of the muscle belly. Once the muscle has converted to fatty tissue, it does not regenerate even after a successful repair. Patients with long-standing tears often have less strength recovery potential than those who receive early surgical intervention.
Number of tendons torn directly affects recovery length. Single-tendon repairs involving the supraspinatus (the most common) have the fastest recovery and best outcomes. Repairs involving two or more tendons (supraspinatus and infraspinatus, for example) extend timelines and carry higher re-tear risk.
Warning Signs: When Your Recovery Is Not Going as Expected
Rotator cuff recovery is long, but it follows a broadly predictable arc. Certain symptoms fall outside that arc and require prompt contact with the surgical team.
Sudden severe pain after a period of improvement is the most important warning sign. If a patient has been progressing through physical therapy and experiences a sharp, escalating pain event, often associated with reaching or lifting, the repair may have failed. This warrants an urgent call to the surgeon, not a wait-and-see approach.
A pop or tearing sensation during activity, even minor activity like reaching into a cabinet, is a potential re-tear signal and should be reported the same day.
Fever, increasing redness, warmth, or drainage at the incision sites in the first two weeks post-surgery indicate possible wound infection. Deep shoulder infections after arthroscopic surgery are uncommon but serious, and early antibiotic treatment makes a significant difference in outcomes.
Stiffness that worsens rather than improves after week 8 may indicate adhesive capsulitis. Post-surgical frozen shoulder is a recognized complication that responds to specific physical therapy protocols and, in some cases, a corticosteroid injection or manipulation under anesthesia. It does not resolve on its own.
Weakness that fails to progress despite consistent physical therapy past the 4-month mark should prompt a conversation about repeat imaging. Johns Hopkins Medicine notes that failed rotator cuff repairs often present as persistent weakness without sharp pain, distinguishing them from normal post-surgical fatigue.
If any of these signs appear, a physician evaluation is the right next step. Use Momentary Lab's doctor finder to locate an orthopedic specialist or shoulder surgeon near you who can assess the recovery and order imaging if needed. For broader guidance on navigating care options and understanding your shoulder health, Momentary Lab's AI healthcare navigator can help you find reliable information quickly.
Is Rotator Cuff Surgery Worth It? Setting Honest Expectations
The question of whether to pursue rotator cuff surgery is one of the most commonly searched questions among patients with confirmed tears, and it deserves a direct, evidence-based answer.
For small and medium tears repaired in patients under 65 with good tissue quality and no significant comorbidities, patient satisfaction rates are high. Published data referenced through PubMed studies on rotator cuff repair outcomes document satisfaction rates of 85 to 95% in this population at two-year follow-up.
For larger tears and older patients, satisfaction rates remain meaningful, generally in the 70 to 85% range, but expectations for full strength recovery need to be more conservative. The goal shifts from "returning to exactly where I was before" to "regaining enough function to live and work without chronic pain."
What happens if a torn rotator cuff is left untreated? Partial tears frequently progress to full-thickness tears over time. Full-thickness tears, once present, rarely shrink. As the tendon retracts, fatty infiltration of the muscle belly increases, and that fatty degeneration is not reversible even after a later surgical repair. Patients who delay surgery often find that when they eventually proceed, the repair is technically more difficult and the functional outcome ceiling is lower. The Cleveland Clinic advises that timing of surgical intervention matters, particularly for younger and more active patients.
Surgery is not always the right answer. Partial tears in older, low-demand patients are often managed successfully with physical therapy, corticosteroid injections, and activity modification. But for full-thickness tears in patients who want to remain active, the evidence supports surgical repair when tissue quality and overall health allow it.
Practical Daily-Life Guide for Recovery at Home
The hospital discharge paperwork covers wound care and medication schedules. What it often does not cover is the texture of daily life for the next several months. This section fills that gap.
Sleep position is one of the most frequent patient complaints in the first four to six weeks. The best option for most patients is a recliner or an adjustable bed elevated to 30 to 45 degrees. This position reduces pressure on the shoulder joint and prevents the arm from rotating internally during deep sleep. If neither is available, a three-pillow arrangement (one under the head, one under the surgical arm, one tucked against the ribcage to prevent arm rollover) mimics the same angle on a flat bed. Expect disrupted sleep for at least the first four weeks; this is nearly universal.
Showering requires keeping the incision sites dry for the first 48 to 72 hours. After that, a waterproof wound cover (available at any pharmacy) allows a brief shower with the arm held close to the body. Full overhead showering typically waits until the sling is fully discontinued. A handheld showerhead and a shower seat reduce fall risk and fatigue in the early weeks.
Dressing with one arm is more manageable with the right wardrobe choices. Oversized button-front shirts, elastic-waist pants or shorts, slip-on shoes, and front-clasp bras eliminate most of the frustration. Thread the surgical arm through sleeves first when dressing; remove it last when undressing.
Driving logistics depend on which arm was operated on, whether the vehicle is automatic or manual, and pain medication status. Narcotic pain medications prohibit driving entirely. For most automatic-transmission vehicles with non-dominant arm surgery, driving clears around 2 to 4 weeks. Dominant-arm surgery generally waits until 4 to 6 weeks.
Nutrition during recovery is worth intentional planning. Adequate protein (lean meats, eggs, legumes, Greek yogurt) supports collagen synthesis. Anti-inflammatory foods like fatty fish, olive oil, berries, and leafy greens may support the healing environment. Hydration directly affects tissue healing and energy levels during rehabilitation.
Mental health during a long recovery is a legitimate concern that tends to be underaddressed in clinical settings. Rotator cuff surgery recovery is isolating, particularly for athletes or physically active individuals who define a significant part of their identity through sport or labor. Feeling frustrated, depressed, or anxious about slow progress at the 3 to 4-month mark is common and does not indicate weakness. Acknowledging it early, finding low-impact activities that are cleared (walking, stationary cycling once cleared, meditation), and maintaining social connection during the recovery period improves both mental and functional outcomes.
Frequently Asked Questions
How painful is recovering from rotator cuff surgery?
The first two weeks are typically the most uncomfortable, with sharp pain at the incision sites and deep aching from inflammation around the repair. Most patients manage this with a short course of prescribed pain medication, transitioning to over-the-counter options around week 2 to 3. Physical therapy in weeks 6 through 12 can be intense as the capsule is stretched, but the pain during this phase is different in character, more of a deep stretch than acute surgical pain. By month 4, most patients describe the shoulder as mildly uncomfortable after activity rather than acutely painful at rest.
What are the worst things to do after rotator cuff surgery?
Removing the sling too early, performing active shoulder exercises before the surgeon clears them, returning to overhead lifting before the 12-week threshold, and resuming heavy labor or contact sports without formal clearance are the most common and consequential mistakes. Smoking during recovery, skipping physical therapy, and sleeping on the surgical arm without positional support also negatively impact outcomes.
Is rotator cuff surgery considered a major surgery?
It is a significant surgical procedure with a long recovery, but it is most often performed arthroscopically through small incisions rather than open incision, which reduces hospital stay (most patients go home the same day), infection risk, and tissue trauma compared to open surgery. The complexity of the repair, not just the technique, determines recovery length. A massive four-tendon tear requiring augmentation is a substantially more involved procedure than a small single-tendon repair.
How long should I rest after rotator cuff surgery?
Complete rest of the shoulder is required for the first 4 to 6 weeks. This does not mean bed rest for the whole body; walking and lower-body activity are encouraged early. The shoulder specifically must be protected from active loading until the surgeon clears passive motion, and from resistance exercise until the 12-week biological threshold. Returning to rest-only after that window slows recovery. Structured physical therapy, not extended rest, drives the strengthening phase.
When can I drive after rotator cuff surgery?
Non-dominant arm surgery with an automatic transmission vehicle typically clears for driving at 2 to 4 weeks, provided the patient is off narcotic pain medication. Dominant-arm surgery generally waits until 4 to 6 weeks. Long driving trips should be avoided until the sling is fully discontinued, as sustained arm positioning in a vehicle seat can stress the repair.
What is the re-tear rate after rotator cuff surgery?
Overall re-tear rates in the published literature range from 15 to 21%. Re-tear risk is substantially higher for massive tears (over 5 cm), patients over age 65, smokers, and patients with significant preoperative fatty infiltration. Small tear repairs in younger patients can carry re-tear rates below 10%. Most re-tears occur in the first 3 months, during the biological consolidation window when the repair is most vulnerable to loading.
References
- Galatz LM et al., PMC / National Institutes of Health — Cited for the biology of tendon-to-bone healing phases and timeline of structural consolidation.
- PMC / NIH Study on Rotator Cuff Vascularization — Cited for the hypovascular nature of tendon-bone junctions and its role in extended recovery.
- Johns Hopkins Medicine: Failed Rotator Cuff Repairs — Cited for full strength recovery timeline (~9 months) and presentation of failed repairs.
- Cleveland Clinic: Shoulder Arthroscopy — Cited for return-to-sport timelines and the importance of surgical timing.
- PubMed: Rotator Cuff Outcomes Study — Cited for long-term patient-reported outcomes and normal residual symptoms at one year.
- PubMed: Smoking and Rotator Cuff Healing — Cited for smoking as a modifiable risk factor increasing re-tear rate and impairing tendon-to-bone healing.



