
If you're reading this at 2 a.m. with a sling on your arm and a pillow propped under your shoulder, this guide is for you. Most online articles tell patients to "expect some discomfort" and then stop talking around the three-month mark. But research published in peer-reviewed journals shows that the average full recovery from rotator cuff repair takes closer to 14 months, and the gap between what patients are told and what they actually experience is where a lot of unnecessary anxiety lives.
This is the guide your surgeon didn't have time to give you in a 15-minute appointment.
At a Glance
| Topic | Key Facts |
|---|---|
| Typical pain duration | 3 to 6 months for most daily activity; up to 14 months for full recovery |
| Worst pain window | Days 1 to 3 after nerve block wears off; weeks 1 to 4 of sling phase |
| Night pain resolution | Most patients see improvement by 3 to 6 months post-op |
| Surgery type matters | Arthroscopic repair generally shows better pain and healing outcomes than open surgery |
| Healing phases | Inflammatory (0 to 6 wk), proliferative (6 wk to 3 mo), remodeling (3 to 12+ mo) |
| When to call your surgeon | Fever above 101.5°F, sudden severe pain after progress, redness or warmth at incision site |
The Honest Truth: Why Rotator Cuff Surgery Hurts (and When It Gets Better)
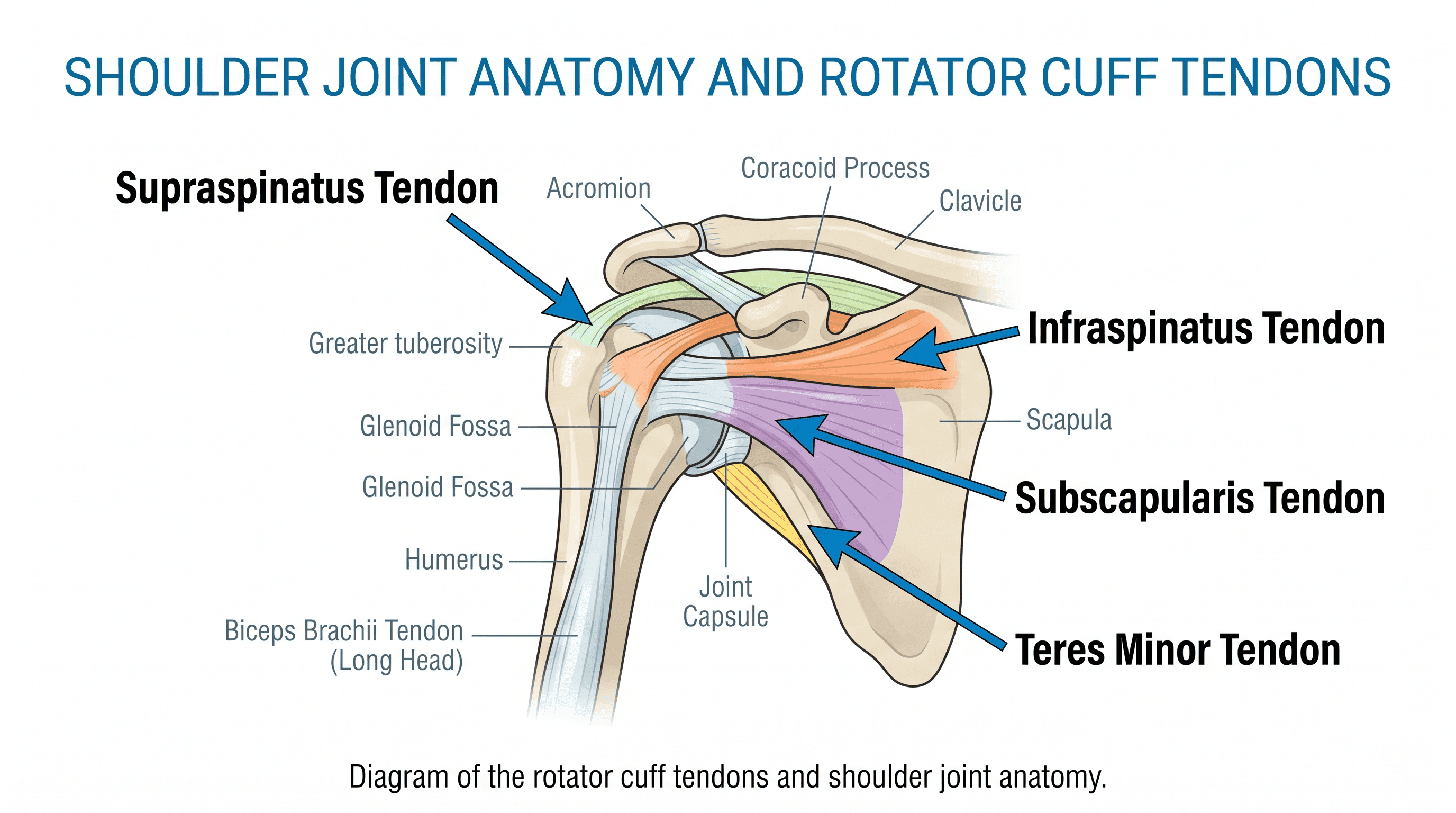
Rotator cuff surgery is not a minor procedure, and pain after shoulder surgery is both expected and biologically necessary. The rotator cuff is a group of four muscles and their tendons that surround the shoulder joint, stabilizing it and allowing overhead movement. When one or more of those tendons tears and is repaired surgically, the body has to rebuild the tendon-to-bone attachment from scratch, a process that unfolds across overlapping biological phases spanning many months.
The honest answer to "how long will I have pain after rotator cuff surgery" is: most of the sharp, constant pain resolves by weeks six to twelve. The dull aching that follows physical therapy and activity fades between months three and six. But a meaningful minority of patients, especially those with larger tears or older age, carry some degree of residual discomfort through the twelve- to fourteen-month mark.
Here is a high-level timeline to orient you before going deeper into each phase.
| Phase | Timeframe | What Pain Feels Like |
|---|---|---|
| Nerve block rebound | Days 1 to 3 | Sudden, sharp, burning after anesthesia fades |
| Peak acute pain | Weeks 1 to 4 | Constant deep ache; worse with any movement |
| Transition pain | Weeks 4 to 8 | Stretching soreness from PT; movement stiffness |
| Strength-phase ache | Months 3 to 6 | Dull fatigue ache after activity; overhead sensitivity |
| Final stretch | Months 6 to 14 | Intermittent aching; weather sensitivity; functional plateau |
Why Rotator Cuff Surgery Hurts More Than You Expect
The Biology of Tendon Healing
Tendon-to-bone repair does not heal the way a cut on your skin heals. According to Johns Hopkins Medicine, initial bone attachment begins forming at around six weeks, a stronger bond develops by three months, and true tendon integration into the bone is not complete until six to nine months post-operatively. This biological timeline is not negotiable. Pain persists in part because the tissue is structurally incomplete, and the body is actively remodeling it.
The healing process moves through three overlapping phases: the inflammatory phase (zero to six weeks), the proliferative phase (six weeks to three months), and the remodeling phase (three months to well over a year). Each phase has its own pain signature, which is why recovery does not feel like a straight line downward.
The Role of Post-Surgical Stiffness in Prolonging Pain
Sling immobilization is protective, but it comes with a side effect: the shoulder joint capsule stiffens from disuse, and that stiffness amplifies perceived pain significantly. When the arm is held in one position for weeks, inflammation accumulates around the joint capsule and the surrounding bursa. Patients often describe this as a sensation of tightness or pressure that sits underneath the surgical pain itself.
This is why many patients feel pain getting worse around weeks two to four even as the incision heals. The stiffness is doing its job of protecting the repair, but it creates a secondary pain source that physical therapy will address in the weeks that follow.
Pain by Phase: What You Will Feel Week by Week
Days 1 to 3: The Nerve Block Wears Off
Most rotator cuff surgeries are performed under general anesthesia combined with a regional nerve block, typically an interscalene block, that numbs the entire arm and shoulder for anywhere from twelve to twenty-four hours. The first day after surgery often feels surprisingly manageable because the block is still active.
The rebound hits when it wears off. This is consistently the most jarring moment in the early recovery, and patients who are not prepared for it often describe feeling blindsided. The pain that emerges is sharp, burning, and often described as the worst of the entire recovery. Staying ahead of it with prescribed medication, rather than waiting until pain is already severe, is the single most important pain management move in this window.
Weeks 1 to 6: The Sling Phase
This is the period of constant, deep aching. The arm sits in a sling twenty-four hours a day (or close to it, with surgeon-specific variation), and even small movements, a cough, a sneeze, rolling over in bed, can send a sharp jolt through the shoulder. Visual analog scale (VAS) pain scores at six weeks after rotator cuff repair average around 4 out of 10 according to published surgical outcomes data, which translates in practical terms to pain that is always present but manageable with medication and ice.
Cold therapy is particularly valuable in this phase. Motorized ice machines (sometimes called cryo-cuffs or cold therapy units) circulate cold water through a shoulder wrap and are widely recommended by orthopedic surgeons for continuous use in the first two to four weeks. They are more effective than gel ice packs for sustained cold application without the risk of skin damage from direct ice contact.
Weeks 4 to 8: Physical Therapy Begins
Between weeks four and eight, most surgeons begin passive range-of-motion exercises, meaning a physical therapist moves the arm for the patient rather than having the patient use their own muscle force. This transition introduces a new kind of pain: the stretching, pulling soreness of a stiff joint being asked to move again.
This phase confuses many patients because they expected pain to be decreasing, and instead they feel a new variety of discomfort. But this soreness is different from surgical pain. It has a directional quality (felt at the end of a stretch), it peaks during therapy and fades within an hour, and it is a sign that the shoulder is responding to treatment. Persistent, sharp, or worsening pain after a PT session is a different matter and warrants a call to the surgical team.
Months 3 to 6: Rebuilding Strength
By three months, most patients have graduated from passive motion to active-assisted motion and then to light strengthening exercises. VAS scores drop to roughly 3 out of 10 at three months and closer to 1.5 out of 10 by six months for patients with good healing trajectories. The character of pain in this phase shifts again, from a constant ache to a fatigue-type soreness that shows up after activity and eases with rest.
Overhead reaching remains uncomfortable for most patients through this phase. Sleeping on the operated shoulder is typically not yet comfortable. But daily activities like typing, light carrying, and driving (once the surgeon clears it) become increasingly manageable.
Months 6 to 14: The Phase Nobody Warns You About
Here is what most recovery guides do not tell you: a 2019 study with 135 patients found that average time to full recovery after rotator cuff repair was approximately 14 months. Yet most patient-facing content implies the hard part ends at six months. The result is a large population of patients at month eight or ten who feel they are failing recovery because they still have pain, when they are actually progressing normally.
The pain in this final stretch is intermittent rather than constant. It tends to show up with overhead lifting, repetitive activity, or weather changes. Strength asymmetry between the operated and non-operated shoulder may persist. Some patients notice a kind of "awareness" in the shoulder, a low-grade sensitivity that is not exactly pain but is not gone either. This is normal, and it does continue to improve with consistent home exercise.
Night Pain After Rotator Cuff Surgery: Why It Is So Bad and How to Sleep
Why Shoulder Pain Spikes at Night
Night pain is one of the most distressing parts of rotator cuff recovery, and it is almost universally underaddressed in the information patients receive before surgery. The mechanisms behind it are real and well-documented.
When lying flat, the shoulder loses the benefit of gravity-assisted drainage, and fluid accumulates around the inflamed joint capsule. Blood flow in the anterior humeral circumflex artery (the primary vessel supplying the humeral head) increases when horizontal, which amplifies inflammatory signaling at the surgical site. There is also an emerging body of research on the role of melatonin receptors in joint tissue. Synovial cells express melatonin receptors, and nighttime melatonin surges appear to upregulate inflammatory cytokines including IL-6, increasing pain sensitivity precisely when patients are trying to sleep.
How Long Does Night Pain Last After Surgery?
Research published in 2022 in the American Journal of Sports Medicine found that approximately 90% of rotator cuff repair candidates report sleep disturbance before surgery due to shoulder pain. The good news is that the majority of patients see meaningful improvement in sleep quality by three to six months post-operatively, with continued gradual improvement through the first year. Patients who still have significant night pain at six months warrant a conversation with their surgeon about the possibility of incomplete healing or secondary conditions.
Best Sleep Positions and Practical Fixes
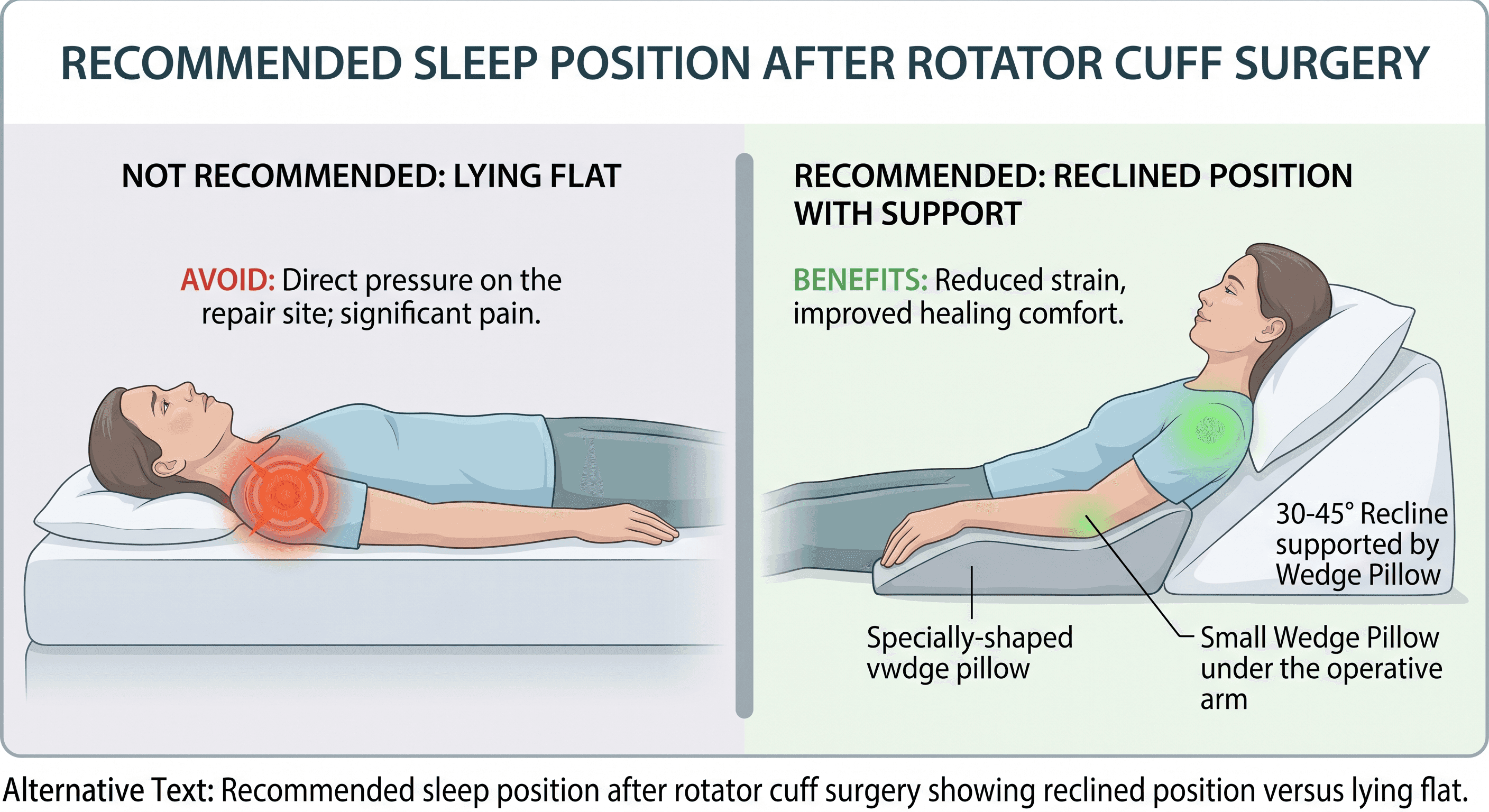
The single most effective change most patients can make is sleeping in a recliner or propped at a 30 to 45-degree angle rather than lying flat. This position keeps gravity working in the right direction and reduces fluid accumulation around the joint.
If a recliner is not available, stacking pillows to achieve a similar incline on the bed works reasonably well. A wedge pillow under the operated arm, providing support underneath the elbow and forearm, takes tension off the shoulder capsule. Whether to wear the sling during sleep is a surgeon-specific decision, but many orthopedic surgeons recommend it for the first four to six weeks of recovery to prevent unconscious repositioning during sleep.
Factors That Change How Long Your Pain Lasts
Tear Size and Tendon Quality
Tear size is one of the strongest predictors of recovery length and pain trajectory. Small tears (under 1 cm) carry a healing rate of approximately 96% and follow a relatively predictable timeline. Large tears (over 3 cm) and massive tears show complete healing rates closer to 58%, according to research on failed rotator cuff repairs from Johns Hopkins Medicine. Patients with larger tears should expect a longer pain course and greater variability in outcomes.
Arthroscopic vs. Open Surgery
Arthroscopic rotator cuff repair, in which the surgery is performed through small incisions using a camera and miniature instruments, generally produces better outcomes than traditional open surgery on metrics including pain, healing time, and post-operative function. Published 2024 research comparing arthroscopic and open cohorts found the arthroscopic group showed improved outcomes across pain scores and functional recovery. The choice of technique depends on tear characteristics, and a doctor can advise on which approach is appropriate for an individual case.
Age and Muscle Quality
Healing rates decline measurably with age. Patients under 50 show rotator cuff healing rates around 87.8%, while patients over 61 drop to approximately 65.4%, according to data reviewed by the National Center for Biotechnology Information. Fatty degeneration of the rotator cuff muscle belly, graded on a scale during pre-operative MRI, also predicts healing and pain duration. Higher grades of fatty degeneration are associated with increased re-tear rates and slower functional recovery.
This is not a reason to avoid surgery. It is context for building a realistic timeline.
Smoking, BMI, and Lifestyle Factors
Smoking is consistently associated with longer recovery timelines and higher rates of complications after orthopedic procedures, including rotator cuff repair. Patients who smoke before or during recovery may experience slower tendon-to-bone healing and more persistent pain. Elevated BMI places additional mechanical load on the healing shoulder. Neither is a disqualifier for surgery, but both are modifiable factors worth discussing with the surgical team before and after the procedure.
How to Manage Pain During Recovery
Medications: What Is Prescribed and for How Long
Most surgeons prescribe a short course of opioid pain medication for the immediate post-operative period, typically three to seven days, combined with scheduled non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen. NSAIDs address the inflammatory component of pain and are often continued for several weeks. Some surgeons also prescribe a short steroid taper or a longer-acting nerve block that can be placed at the time of surgery.
Taking pain medication on a schedule in the first week, rather than waiting for pain to become severe before dosing, is considerably more effective for keeping acute pain controlled. A doctor can advise on the appropriate medication plan based on individual health history.
Ice and Heat: Timing Matters
Cold therapy reduces inflammation and numbs the area; it is most effective in the first four to six weeks. After that window, once the acute inflammatory phase has subsided, heat can help relax stiff musculature around the shoulder before physical therapy sessions. Using heat before PT and ice after PT is a pattern many physical therapists recommend during the middle phases of recovery.
Physical Therapy as Pain Management
Physical therapy after rotator cuff repair is not only about regaining range of motion and strength. Targeted manual therapy, joint mobilization, and soft tissue work performed by a skilled PT actively reduces pain by addressing the secondary stiffness and muscle guarding that develops around the surgical site. Patients who are consistent with their PT program consistently show faster pain resolution than those who are not.
A Note on Opioids and Recovery
Emerging evidence from 2022 to 2024 suggests that limiting opioid use around the time of rotator cuff surgery may actually improve long-term pain outcomes. Prolonged opioid use is associated with increased central pain sensitization, a process by which the nervous system becomes hyperresponsive to pain signals over time. Patients who complete the acute opioid phase and transition to non-opioid pain management earlier tend to report better sleep quality and lower overall pain scores at the three- and six-month marks. This is an evolving area, and a doctor should guide individual decisions about pain medication duration.
When to Call Your Orthopedic Surgeon
Understanding the difference between normal post-operative discomfort and a genuine warning sign is one of the most useful things a patient can know. The table below is not a diagnostic tool, and a doctor should evaluate any symptom that causes concern.
| Expected and Normal | Requires a Call to Your Surgeon |
|---|---|
| Aching and soreness at the surgical site | Fever above 101.5°F at any point after discharge |
| Stiffness in the first four to six weeks | Sudden severe increase in pain after a period of improvement |
| Soreness after physical therapy sessions | Redness, warmth, or discharge at the incision site |
| Occasional sharp pain with movement | Significant swelling of the hand or arm below the sling |
| Night pain that is improving gradually | Pain that has not changed at all after twelve weeks of consistent PT |
| Fatigue in the shoulder during strengthening | New onset of numbness or tingling in the hand or fingers |
If the concern is a possible re-tear, the most reliable diagnostic step is an MRI of the shoulder. Signs of re-tear often include a return of significant weakness, a distinct pop or giving-way sensation, and sharp pain after a period of meaningful improvement. Johns Hopkins Medicine notes that not all re-tears require immediate revision surgery; the appropriate treatment depends on tear characteristics and functional impact, which a specialist is best positioned to assess.
If you are unsure whether what you are experiencing is within normal range, find an orthopedic specialist near you who can review your imaging and recovery progress directly.
The Emotional Side of Rotator Cuff Recovery
No guide to rotator cuff surgery pain is honest if it does not address the emotional weight of this recovery. Nine to fourteen months is a long time to be limited, and the psychological dimension is real.
Many patients, particularly those who are active, athletic, or physically active at work, experience a form of identity disruption during recovery. The inability to do things that define how they spend their time, whether that is swimming, playing with grandchildren, or simply sleeping without pain, accumulates in ways that are hard to predict before surgery. Research consistently links poor sleep quality during recovery to elevated pain scores and increased anxiety, creating a feedback loop that is frustrating precisely because it feels circular.
What patients going through this phase should know: the frustration, the impatience, the moments of real sadness about what the shoulder cannot do yet, are not signs of weakness or failure. They are a rational response to a long, physically demanding recovery. Patients who acknowledge this experience, rather than pushing through it alone, consistently do better. Talking to a physical therapist, a surgeon, or a mental health professional about the emotional dimension of recovery is not separate from healing. It is part of it.
Frequently Asked Questions
Should I still have pain 8 weeks after rotator cuff surgery?
Yes, pain at eight weeks is within normal range for most patients. At eight weeks, the tendon-to-bone repair is still in the early proliferative phase of healing, and physical therapy is just beginning to introduce active motion. VAS scores at six to eight weeks typically average around 3 to 4 out of 10. If pain is severe, getting worse rather than better, or accompanied by new symptoms such as fever or significant swelling, that warrants a call to the surgical team.
What are the worst things to do after rotator cuff surgery?
The most damaging things a patient can do in the early recovery period are removing the sling prematurely, lifting anything heavier than a coffee cup before the surgeon clears it, skipping physical therapy sessions, and sleeping flat on the back without elevation. In the later phases, pushing through sharp pain during strengthening (as opposed to normal exercise soreness) and returning to overhead sport before the surgeon gives clearance are the most common contributors to re-tear.
What is the hardest part of rotator cuff surgery?
Most patients and clinicians point to two distinct phases as the hardest. The first is the nerve block rebound in days one to three, which catches many patients off guard in its severity. The second, perhaps more emotionally difficult phase, is the "last 20%" between months six and fourteen, when progress slows, return to full activity feels perpetually just out of reach, and the recovery no longer looks dramatic to anyone on the outside. Being prepared for both phases in advance makes both more manageable.
Does lingering pain at month eight or ten mean my repair failed?
Not necessarily. A 2019 study of 135 patients found that average full recovery took approximately 14 months, meaning pain or limitation at month eight is statistically typical, not a sign of failure. A failed repair or re-tear has specific characteristics: a sudden return of weakness, a new popping or giving-way sensation, or pain that increases sharply after a period of genuine improvement. Gradual, slowly improving pain is consistent with normal healing.
Will I be completely pain-free after recovery?
The majority of patients who undergo rotator cuff repair do reach a state of functional, daily life that is essentially pain-free. A smaller subset, particularly those with massive tears, significant fatty degeneration, or revision repairs, may retain some degree of activity-related soreness long term. Cleveland Clinic notes that surgery outcomes are strongly tied to the size and severity of the original tear, meaning realistic expectations should be set in conversation with the surgical team before the procedure.
Does arthroscopic surgery hurt less than open surgery?
In general, yes. Arthroscopic repairs involve smaller incisions, less disruption of surrounding muscle tissue, and lower rates of post-operative infection, all of which contribute to a faster and less painful early recovery. Beyond the immediate post-operative period, outcomes data favors arthroscopic repair in terms of pain scores and functional recovery. However, some tear characteristics, particularly very complex or massive tears, may still require open or mini-open techniques, and a doctor can advise on which approach applies to a specific case.
For personalized guidance on understanding your symptoms and navigating your care options, Momentary Lab's AI Healthcare Navigator can help point you in the right direction.
References
- Johns Hopkins Medicine: Failed Rotator Cuff Repairs — Cited for tendon healing timeline, tear size and healing rates, and re-tear evaluation guidance.
- National Center for Biotechnology Information (PMC3094637) — Cited for age-stratified healing rates and fatty degeneration data.
- Cleveland Clinic: Shoulder Arthroscopy — Cited for general arthroscopic surgery outcomes and post-operative expectations.
- PubMed (PMID 28131695) — Cited for pre-operative sleep disturbance prevalence and post-operative night pain resolution timeline.



