
The short answer is: it depends on factors most patients never hear about. Whether a meniscus tear ends in the operating room or in a physical therapy gym comes down to how the tear happened, where it sits inside the knee, and what your body has been telling you since the injury. This guide walks through the exact decision framework orthopedic surgeons use, what the most current research says, and how to know when conservative treatment has genuinely run its course.
At a Glance
| Topic | Key Facts |
|---|---|
| Primary keyword | How to know if a meniscus tear needs surgery |
| Who is most affected | Athletes, adults over 40, anyone with a twisting knee injury |
| Red flag symptoms | Knee locking, giving way, inability to fully extend |
| Most decisive factor | Tear type (traumatic vs degenerative) and location (red vs white zone) |
| Conservative treatment window | 8 to 12 weeks before surgical re-evaluation |
| Surgery types | Meniscus repair (stitching) vs partial meniscectomy (trimming) |
| 2024 research finding | No significant outcome difference between surgery and PT for degenerative tears at 5-year follow-up |
Not All Tears Require the Operating Room
Here is the first thing most patients are not told: a positive MRI is not a surgery prescription. Age, activity level, tear type, and location inside the knee are the variables that drive the treatment decision, not the scan result alone.
The Cleveland Clinic notes that many people with meniscus tears manage well with non-surgical care, particularly when symptoms are mild and mechanical stability is preserved. For degenerative tears in adults over 40, physical therapy alone often delivers outcomes equivalent to arthroscopic surgery over a 5-year period, based on a 2024 meta-analysis published in peer-reviewed orthopedic literature.
Traumatic tears in younger, active patients tell a different story. A sudden force that creates a large, unstable tear in a 25-year-old soccer player carries a very different surgical calculus than gradual cartilage wear in a 62-year-old with mild knee stiffness.
So before asking whether surgery is necessary, the more useful question is: what kind of tear do I have, and what is it doing to my knee right now?
The Absolute Red Flags: Mechanical Symptoms That Warrant Urgent Referral
Mechanical symptoms are the clearest signal that surgery may not be optional. They indicate that something physically unstable is inside the joint, not just something painful.
The three red flags that push a meniscus tear toward urgent surgical evaluation are:
Knee locking occurs when a displaced fragment of cartilage physically blocks the knee from straightening. A locked knee cannot be fully extended, and forcing it causes sharp pain. This is not stiffness after rest. It is a structural block, and it typically signals a bucket handle tear (covered in the next section).
Giving way or buckling describes a knee that suddenly collapses under body weight with no warning. This indicates mechanical instability, meaning the joint is no longer reliably load-bearing. It carries a risk of secondary injury to surrounding ligaments and cartilage.
Catching or clicking with pain is distinct from the harmless pops many people feel in their knees. When catching is painful and recurs consistently during specific movements, it suggests a loose or displaced tissue fragment is interfering with normal joint mechanics.
The Mayo Clinic identifies inability to move the knee through its full range of motion as a key clinical indicator that warrants prompt medical evaluation. If any of these mechanical symptoms are present, watchful waiting is not the recommended path.
"Locked knee, giving way, and a block to full extension are the clearest clinical signals that a meniscus tear may require surgical correction rather than conservative management." Mayo Clinic
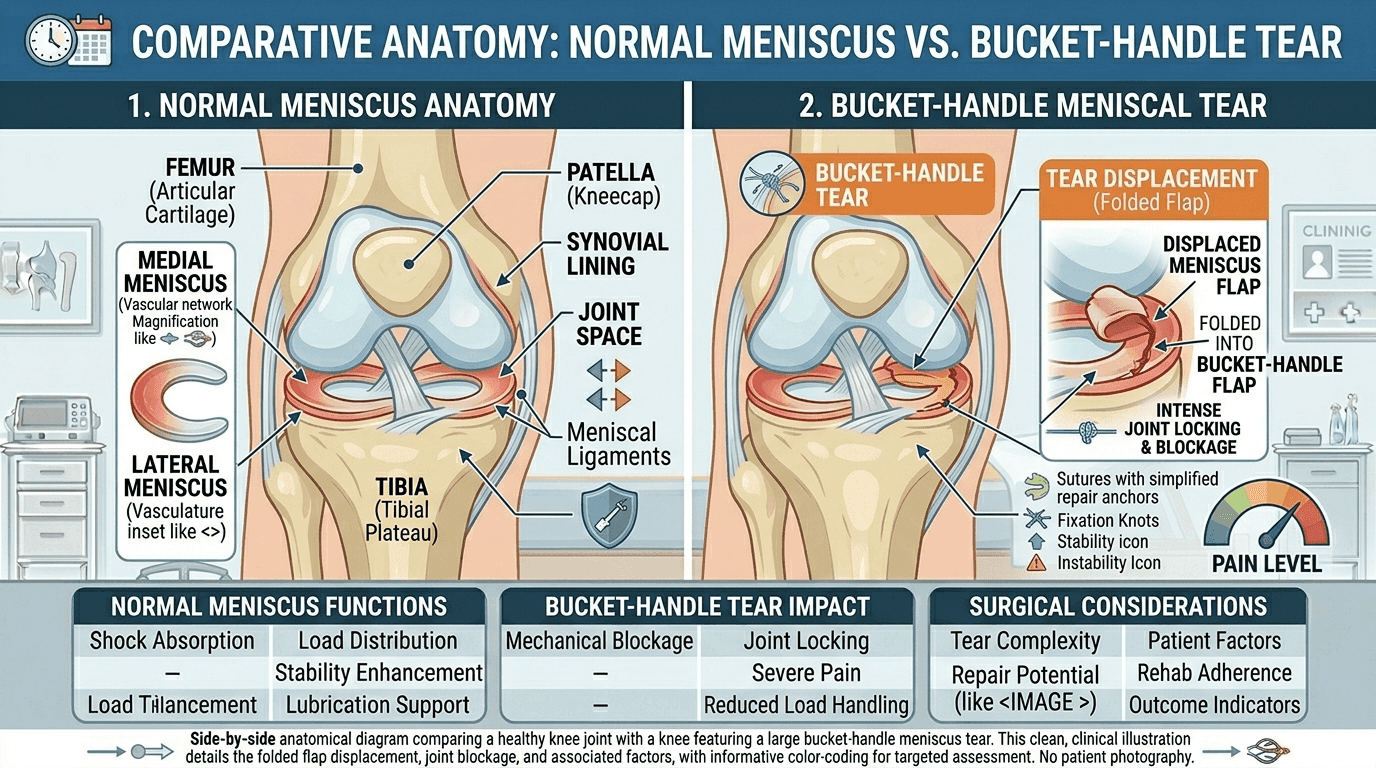
The Bucket Handle Tear: When the Knee Literally Cannot Straighten
A bucket handle tear is a specific tear pattern that deserves its own section because it behaves differently from every other meniscus injury.
In a bucket handle tear, a large, longitudinal flap of meniscal cartilage breaks away but remains partially attached at both ends. That flap then folds, or "flips," into the center of the knee joint like the handle of a bucket folding inward. Once displaced, it physically sits inside the joint space and prevents the knee from fully extending.
This is one of the few meniscus tear patterns where surgery is rarely debated. The mechanical obstruction cannot be resolved with physical therapy or anti-inflammatory medication because there is a structural block inside the joint. According to research indexed on PubMed, bucket handle tears are strongly associated with the need for surgical repair, particularly in younger patients where preserving meniscal tissue is a priority.
Bucket handle tears often occur during high-force rotational injuries, are more common in athletes under 40, and are frequently accompanied by ACL injuries. The classic presentation is a knee that locks suddenly after trauma and cannot straighten past a specific angle regardless of how much the patient tries to extend it.
If an MRI identifies a bucket handle pattern, the surgical conversation typically begins at that appointment, not after a failed course of physical therapy.
Traumatic vs Degenerative Tears: Why the Same Diagnosis Leads to Different Decisions
Two people can walk into an orthopedic clinic with identical MRI findings and leave with completely different treatment plans. The reason is almost always the tear's origin: was it traumatic or degenerative?
Traumatic Tears
A traumatic meniscus tear results from a sudden, high-force event. A hard pivot on a planted foot, a direct blow to the knee, or a jump landing gone wrong are classic mechanisms. These injuries tend to affect younger patients, produce large or complex tears, and create more immediate mechanical symptoms.
Research published via PubMed and reviewed in orthopedic literature supports surgical repair for large traumatic tears in younger patients, particularly when caught early. Repair within three weeks of injury has been associated with lower recurrence risk and better long-term cartilage preservation compared to delayed intervention.
For athletes under 40 with a traumatic tear that has produced instability, locking, or a significant tear pattern, surgery is often the first-line recommendation rather than the fallback.
Degenerative Tears
A degenerative meniscus tear develops over time as cartilage gradually breaks down with age and use. These tears are extremely common in adults over 40 and are frequently discovered incidentally on MRIs ordered for general knee pain.
This is where the research has shifted considerably in recent years. A 2024 meta-analysis found no statistically significant difference in knee function, pain scores, or activity levels between surgery and structured conservative care (physical therapy) for degenerative tears at 5-year follow-up. The NIH research database includes systematic reviews supporting physical therapy as the appropriate first-line treatment for degenerative lesions, particularly in patients with underlying osteoarthritis.
For a 62-year-old with a degenerative tear and no mechanical symptoms, the current evidence strongly supports starting with conservative treatment before considering the operating room.
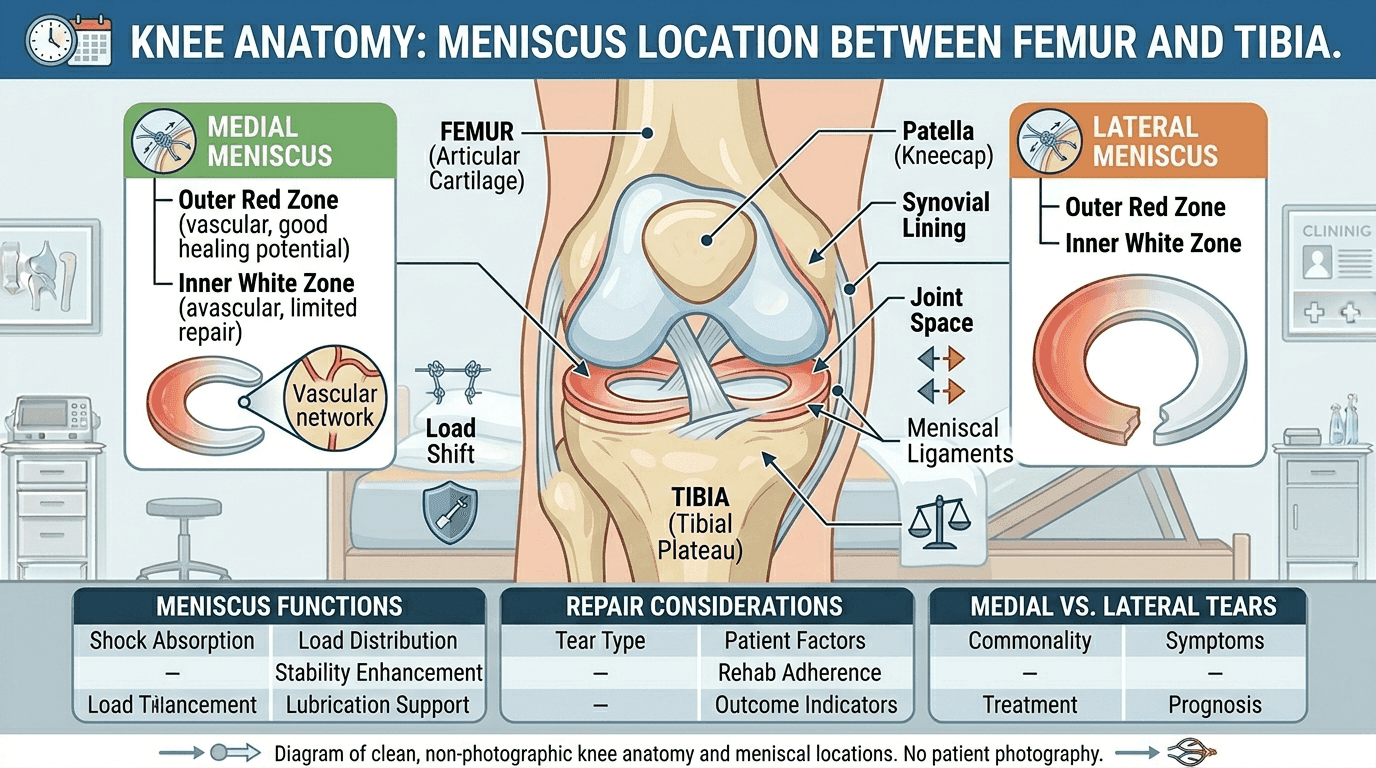
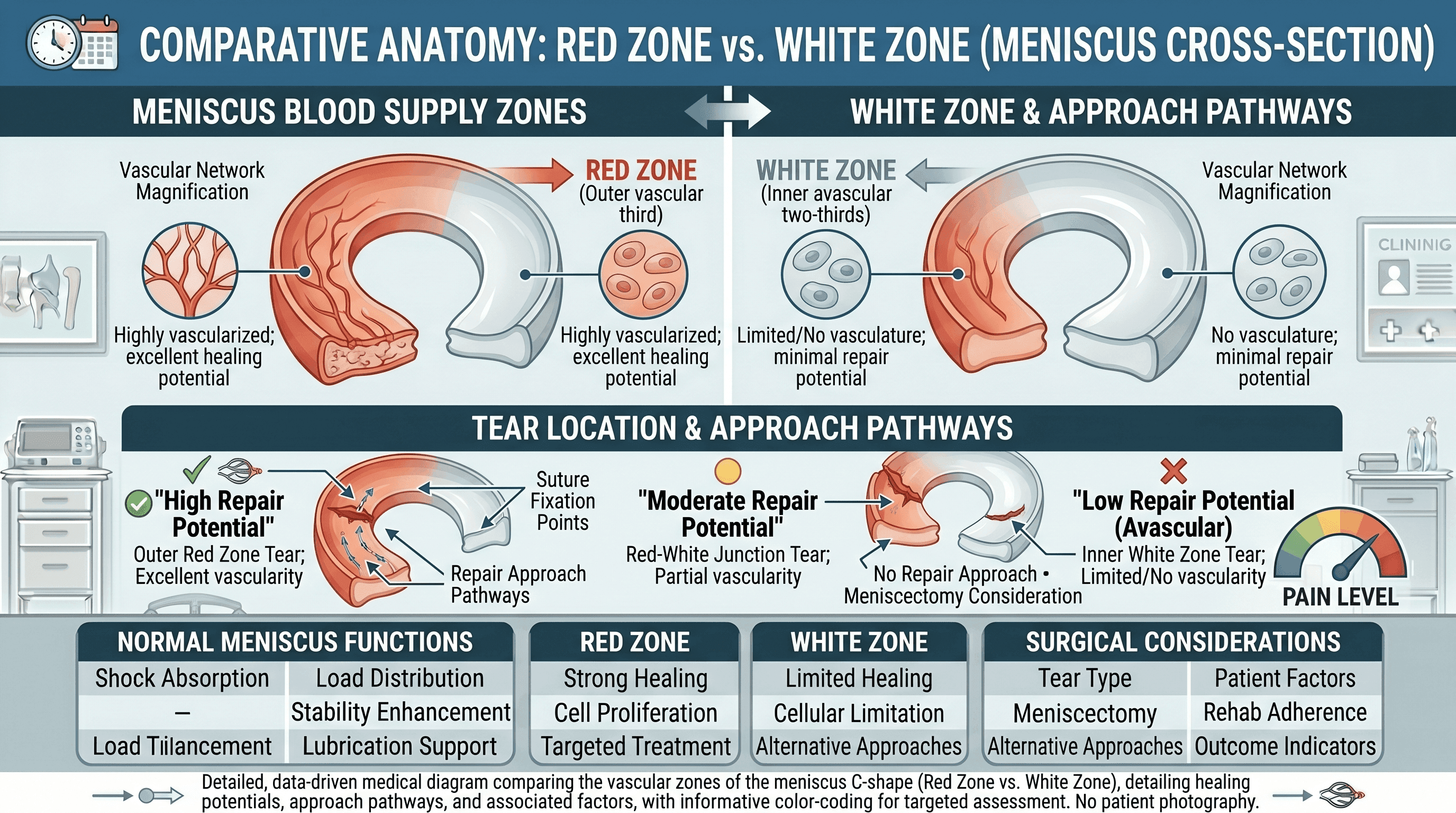
Location, Location, Location: The Red Zone vs White Zone
Where a tear sits inside the meniscus matters as much as what kind of tear it is. The meniscus has two distinct zones defined entirely by blood supply, and that distinction directly controls whether a surgeon can repair the tissue or must simply remove it.
The Red Zone is the outer third of the meniscus. It has a direct blood supply, which means the tissue can receive nutrients, mount a healing response, and knit back together after surgical repair. Tears in the red zone are candidates for meniscus repair, where the surgeon stitches the torn edges back together and allows the tissue to heal over months.
The White Zone is the inner two-thirds of the meniscus. It is avascular, meaning it receives no direct blood supply. Torn tissue here cannot heal on its own and cannot be reliably repaired surgically. When a tear is located in the white zone, the standard surgical approach is partial meniscectomy: trimming away the damaged tissue rather than stitching it.
According to NCBI Bookshelf, tear location relative to vascular supply is one of the primary determinants surgeons use when deciding between repair and meniscectomy. This matters for long-term outcomes because preserving meniscal tissue reduces the risk of future osteoarthritis compared to removal.
A tear in the red zone in a 28-year-old with mechanical symptoms is a very different surgical conversation from a white-zone tear in a 55-year-old with degenerative changes. Same diagnosis on paper; very different paths.
The 5 Factors Your Doctor Weighs When Recommending Surgery
Most surgical recommendations are not made on a single data point. They are the product of five overlapping clinical variables, and understanding each one makes the surgeon's reasoning much easier to follow.
The Mechanical Symptoms Trigger
Knee locking, a block to full extension, and repeated giving way are the highest-weighted factors in the surgical decision. When any of these are present, the threshold for recommending surgery drops considerably because they indicate the tear is mechanically disrupting joint function, not just causing pain. For athletes under 40, these symptoms often warrant urgent referral rather than a trial of conservative care.
Age and Activity Level
Age and activity level are considered together, not separately. A 35-year-old competitive runner with a traumatic tear and an active lifestyle is a strong surgical candidate when conservative treatment fails. A 68-year-old with a degenerative tear, mild symptoms, and no interest in high-impact sport is not. The Mayo Clinic notes that surgery for degenerative tears in older patients with underlying osteoarthritis often shows no meaningful benefit over physical therapy alone. Age is not disqualifying, but it reframes the risk-to-benefit calculation.
Tear Type and Pattern
As covered earlier, traumatic tears with complex patterns (bucket handle, radial, RAMP lesions) carry higher surgical urgency than simple degenerative tears. Tear pattern also determines whether repair or meniscectomy is the appropriate procedure, which affects recovery timelines significantly.
Location in the Red or White Zone
Blood supply determines healing potential. Red-zone tears are repairable; white-zone tears typically are not. Location directly controls which surgical option is available.
Failed Conservative Treatment
Persistent, function-limiting symptoms after 8 to 12 weeks of structured physical therapy, NSAIDs, and appropriate rest define conservative treatment failure. This is not self-assessed. A treating physician or physical therapist should confirm that the patient has completed and genuinely engaged with the program before this threshold is applied.
When a patient who is not a surgical emergency has gone through a full conservative protocol and still cannot perform basic daily activities without pain or instability, surgery moves from a last resort to a reasonable next step.
If you are working through this decision and want to speak with a specialist, find a board-certified orthopedic physician near you who can assess your specific tear pattern, MRI findings, and functional goals before a final recommendation is made.
What the Latest Research Actually Says About Surgery vs No Surgery
The research on meniscus surgery has changed meaningfully over the past decade, and the 2024 evidence base now challenges several assumptions that once made surgery the default choice.
For degenerative meniscus tears, multiple high-quality studies now show that supervised physical therapy produces outcomes equivalent to arthroscopic partial meniscectomy at 5-year follow-up across pain, function, and patient-reported quality of life scores. A systematic review supported by data in the NIH research database reinforces physical therapy as the first-line treatment for degenerative meniscal lesions in middle-aged and older adults. The 2024 European and US meniscus consensus guidelines now formally recommend non-surgical management as the starting point for this population.
For traumatic tears, bucket handle tears, and RAMP lesions in younger patients, the picture is different. These tear patterns carry genuine mechanical risks, and the evidence supports early surgical repair over watchful waiting when instability or locking is present. Research from PubMed documents that repair of certain tear patterns within the first three weeks is associated with better structural outcomes than delayed surgery.
The practical takeaway: if a surgeon immediately recommends surgery for a newly diagnosed degenerative tear in a patient over 50 with no mechanical symptoms and no prior conservative treatment, it is entirely reasonable to ask why a supervised PT trial is not being proposed first. Conversely, if a traumatic bucket handle tear is diagnosed in a 30-year-old with a locked knee, an urgent surgical referral is well-supported by current evidence.
Conservative Treatment: What It Involves and How Long to Give It
Conservative treatment is not simply rest and hope. It is a structured protocol, and its effectiveness depends on actually completing it.
The standard conservative program for a meniscus tear includes: RICE (rest, ice, compression, elevation) in the acute phase; non-steroidal anti-inflammatory drugs (NSAIDs) for pain and swelling management; and a supervised physical therapy program focused on quadriceps strengthening, range of motion restoration, and neuromuscular control of the knee.
Cortisone injections are sometimes used to manage pain and reduce inflammation, but they do not promote cartilage healing. They are a symptom management tool, not a treatment for the underlying structural injury. For older patients with degenerative changes, hyaluronic acid injections offer another pain-management option, though evidence for their long-term efficacy is mixed.
The standard timeline before re-evaluation is 8 to 12 weeks of consistent, supervised therapy. If symptoms persist or worsen after completing a genuine course of conservative care, that is the threshold at which a surgical consultation is appropriate.
One emerging area worth noting is orthobiologics, including platelet-rich plasma (PRP). While research is still ongoing and PRP is not yet a standard-of-care recommendation, early studies suggest it may offer a non-surgical option for certain patients with degenerative changes. This area is worth asking about during a consultation, particularly for patients who want to exhaust non-operative options before committing to surgery.
If Surgery Is Recommended: Repair vs Meniscectomy, and What Is at Stake
When surgery is the right call, the next decision is which procedure, and the distinction matters enormously for long-term joint health.
Meniscus repair involves stitching the torn tissue back together. It is the preferred approach for red-zone tears in younger patients because it preserves the meniscus, which functions as a shock absorber for the joint. Recovery is longer, typically 6 to 9 months before return to sport, but the long-term outcome for joint health is better. The meniscus retains its structural function after healing.
Partial meniscectomy involves trimming and removing the damaged tissue. It is the appropriate choice for white-zone tears where repair is not viable, and it carries a shorter recovery, often 4 to 6 weeks to return to sport or normal activity. The trade-off is long-term risk. Research published via PubMed and documented in the Cleveland Clinic's clinical resources links partial meniscectomy to higher rates of osteoarthritis compared to repair, because removing meniscal tissue reduces the joint's ability to distribute load evenly over time.
For patients who have already had a meniscectomy and are experiencing progressive joint deterioration, meniscal allograft transplantation exists as a reconstructive option, though it is a more complex procedure reserved for specific cases.
Surgeons strongly prefer repair over meniscectomy when tear location and patient age make it technically viable, precisely because preserving tissue is better for the joint over a 10 to 20-year horizon.
What to Expect If Surgery Proceeds
Recovery timelines and outcomes vary by procedure, so setting realistic expectations before surgery prevents a great deal of post-operative frustration.
For partial meniscectomy, weight-bearing often resumes within days, and most patients return to normal daily activity within 2 to 4 weeks. Return to sport is typically 4 to 6 weeks. The overall success rate at 5 years is approximately 80%, though the long-term osteoarthritis risk is higher compared to repair, particularly in patients who undergo significant tissue removal.
For meniscus repair, non-weight-bearing or partial weight-bearing is maintained for 4 to 6 weeks post-surgery, and full return to sport takes 6 to 9 months. The re-tear rate for meniscus repairs is approximately 36% within 2 years, with higher failure rates in older patients and those with degenerative tissue quality. When repair succeeds, however, the long-term joint outcome is substantially better than meniscectomy.
Leaving a significantly unstable or mechanically disruptive tear untreated carries its own risk: progressive cartilage damage, chronic joint instability, and accelerated osteoarthritis are the most documented long-term consequences of deferred treatment for tears that warranted intervention.
5 Questions to Ask Your Orthopedic Surgeon Before Deciding
No competitor blog in this space offers patients an actionable pre-consultation question list. These five questions give any patient the framework to have a genuinely informed conversation before agreeing to a procedure.
Is my tear traumatic or degenerative? This single question reframes the entire conversation. A traumatic tear in a younger patient and a degenerative tear in an older patient are clinically different injuries even when the MRI looks similar. The answer changes the treatment evidence base entirely.
Is the tear in the red zone? Does it have real healing potential? Location determines whether repair is even an option. If the tear is in the white zone, repair is not on the table, and understanding that upfront prevents confusion about why meniscectomy is being proposed.
What happens if I try 8 to 12 weeks of physical therapy first? For patients with degenerative tears and no mechanical symptoms, this question is clinically appropriate based on current evidence. If the surgeon cannot explain why conservative treatment is not a viable first step, a second opinion is reasonable.
Are you recommending repair or meniscectomy, and why? These two procedures have very different long-term implications for joint health. Understanding which is being proposed, and why the surgeon believes it is appropriate for the specific tear pattern and location, is foundational to informed consent.
What is my long-term osteoarthritis risk with each option? This is particularly relevant for younger patients. Meniscectomy reduces the meniscus's shock-absorbing function and is associated with higher rates of degenerative joint disease over time. Knowing this risk relative to the repair option allows patients to weigh long-term joint health against shorter recovery timelines.
For help finding the right orthopedic specialist for your situation, the Momentary Lab AI Healthcare Navigator can guide you toward the right type of care based on your symptoms, location, and coverage.
FAQ
How do I know if my meniscus tear requires surgery? Three symptoms strongly indicate surgical evaluation: knee locking (inability to fully straighten the knee), giving way or buckling under weight, and catching with pain during movement. These mechanical symptoms suggest a structurally unstable tear that physical therapy alone cannot resolve. Tears without mechanical symptoms, particularly degenerative tears in adults over 40, are typically evaluated for conservative treatment first.
Can you recover 100% from a meniscus tear? Recovery outcomes depend heavily on tear type, location, patient age, and treatment method. Many patients treated conservatively or surgically return to full pre-injury activity levels. Meniscus repair, when successful, offers the best functional outcomes because it preserves the joint's natural shock absorber. Partial meniscectomy carries a higher long-term osteoarthritis risk, which may limit certain high-impact activities over time. A doctor can advise on individual cases based on specific tear characteristics.
Is it worth fixing a torn meniscus? For traumatic tears with mechanical symptoms in younger, active patients, surgery is generally worth it based on current evidence, particularly when repair rather than removal is viable. For degenerative tears in older patients without mechanical symptoms, the 2024 research suggests surgery may offer no significant advantage over supervised physical therapy at 5-year follow-up. The decision is always individual, and the value of surgery depends on tear type, patient goals, and whether conservative treatment has already been attempted.
Can I live with a meniscus tear without surgery? Many people do, particularly those with degenerative tears, mild symptoms, and no mechanical instability. A meniscus tear without locking, giving way, or a block to motion can often be managed long-term with physical therapy, activity modification, and symptom management. The risk of leaving a significantly unstable or mechanically disruptive tear untreated is progressive cartilage damage and accelerated osteoarthritis. A physician assessment is necessary to determine which category a given tear falls into.
What is the difference between a Grade 1, 2, and Grade 3 meniscus tear on MRI? MRI grading classifies signal changes within the meniscus. Grade 1 and Grade 2 show internal signal changes within the cartilage that do not reach the surface; these are typically not symptomatic and rarely require intervention. Grade 3 shows the abnormal signal extending to the articular surface, indicating a true tear through the cartilage. Most clinically relevant tears requiring treatment are Grade 3. The grade alone does not determine whether surgery is needed; tear pattern, location, and clinical symptoms matter equally.
How long can you wait before meniscus surgery becomes less effective? For traumatic tears, particularly bucket handle tears requiring repair, earlier surgery is associated with better outcomes. Research suggests repair within three weeks of injury carries a lower recurrence risk than delayed surgery. For degenerative tears without mechanical symptoms, delaying or forgoing surgery entirely may be appropriate. There is no universal deadline, but extended delay in the presence of mechanical symptoms risks progressive cartilage damage to surrounding joint surfaces.
References
- NIH / PMC — Meniscus tear management systematic review — Cited for evidence supporting PT as first-line treatment for degenerative meniscal tears and comparative outcome data.
- Cleveland Clinic — Torn Meniscus — Cited for non-surgical management, surgical options, and long-term OA risk associated with meniscectomy.
- PubMed — Meniscus repair outcomes — Cited for bucket handle tear surgical indications and early repair outcome data.
- NCBI Bookshelf — Meniscus anatomy and vascular supply — Cited for red zone vs white zone anatomy and vascular supply as determinants of surgical approach.
- PubMed — Meniscectomy and osteoarthritis risk — Cited for long-term OA risk associated with partial meniscectomy compared to repair.
- Mayo Clinic — Torn Meniscus Diagnosis and Treatment — Cited for clinical red flags, surgical criteria, and conservative treatment guidance.



