
You've made it through surgery. Now you're home, or nearly there, and someone hands you a discharge sheet with instructions but no map. Nobody told you what Tuesday would feel like, or why Thursday hurts more than Monday did, or whether the exhaustion you're feeling on week two means something has gone wrong.
It hasn't. But you deserve to know what's actually coming.
This guide covers the full knee replacement recovery timeline, day by day and week by week, the way a good physical therapist friend would: honestly, without sugarcoating the hard parts, and with enough detail that nothing catches you off guard. Recovery after total knee arthroplasty (TKA) is demanding. It is also, for the vast majority of patients, completely worth it.
At a Glance
| Topic | Key Facts |
|---|---|
| Surgery type | Total knee arthroplasty (TKA) or partial knee replacement |
| Hospital stay | Same-day discharge or 1 overnight stay (most patients) |
| First weight-bearing | Within hours of surgery, with physical therapist assistance |
| Peak swelling window | Days 7 to 10 |
| Walker to cane transition | Approximately weeks 3 to 4 |
| Driving clearance | Typically 4 to 6 weeks (right leg) or 6+ weeks (left leg) |
| 90-degree flexion goal | Around 2 weeks post-op |
| Full recovery timeline | Up to 12 months |
| Most patients at 1 year | Significantly reduced pain and improved mobility |
What Happens Immediately After Knee Replacement Surgery?
The moment surgery ends, your body begins healing, even if your brain is still catching up.
Most patients receive spinal anesthesia with mild sedation rather than full general anesthesia, which means less nausea and a faster return to alertness. According to Mayo Clinic, the surgery itself typically takes about two hours, though you should plan for a longer total time in the hospital as your care team monitors your recovery from anesthesia.
In the recovery room, or PACU (post-anesthesia care unit), nurses monitor your vital signs, pain levels, and circulation. A nerve block placed before or during surgery will keep significant pain at bay for the first 12 to 24 hours. This is intentional and helpful, but it also means a reckoning is coming: as that block wears off, usually on Day 2, discomfort increases meaningfully. Knowing this in advance removes most of the fear.
Many patients are surprised to learn that walking begins on the day of surgery. Within a few hours of returning from the operating room, a physical therapist will help you stand, shift your weight, and take your first steps with a walker. This early mobilization is not aggressive or punishing. It is one of the most evidence-supported practices in post-operative orthopedic care, and it significantly reduces the risk of blood clots and supports faster functional recovery.
Emotionally, Day 0 tends to produce a strange mix: relief that it's done, grogginess from anesthesia, and a quiet uncertainty about what comes next. That emotional ambiguity is entirely normal.
Day-by-Day: Your First Week After Knee Replacement
This is the section no competitor gives you. Here is what each day actually looks like.
Day 1: Hospital or Same-Day Discharge
Most patients at US hospitals go home the same day or after one overnight stay, depending on their overall health and how surgery went. If you're staying overnight, you'll have physical therapy again in the morning. You'll practice stairs before discharge (even just two or three steps), because stairs are a real-world discharge requirement.
The nerve block is still active on Day 1, which gives you a manageable baseline. Pain may feel like a 3 or 4 out of 10. Use this window wisely: practice the exercises your PT showed you, ice the knee when you're not moving, and keep it elevated above the level of your heart when resting.
If you're going home today, make sure someone is with you. You cannot drive. You will need help getting in and out of the car, navigating steps at home, and preparing meals. Setting up a comfortable recovery station before surgery, a recliner or elevated sleeping surface, a reacher tool, a shower chair, and a week of easy meals, makes Day 1 at home significantly more manageable.
The emotional note on Day 1: shock and relief often arrive together. Some people feel tearful. Some feel strangely calm. Both are fine.
Days 2 to 3: The Peak Pain Window
This is the phase that catches people off guard, and the one most discharge packets gloss over.
As the nerve block fully wears off, usually somewhere in the Day 2 window, pain increases. For many patients, Days 2 and 3 represent the highest pain levels of the entire recovery. A pain score of 5 to 7 out of 10 is common, even with medication on board.
This is not a sign something went wrong. This is your body's inflammatory response doing exactly what it is supposed to do.
Your surgical team will have prescribed a multimodal pain plan: typically acetaminophen, an NSAID like celecoxib if your stomach can tolerate it, and short-term opioids. Take these as prescribed and on schedule rather than waiting until pain peaks. Staying ahead of pain is far more effective than chasing it once it crests.
Ice and elevation are not optional extras during Days 2 to 3. They are frontline pain management tools. Keep the knee elevated, ice for 15 to 20 minutes at a time, and protect the skin with a cloth barrier to avoid frostbite.
Days 4 to 7: Turning the Corner
Most patients notice a perceptible shift somewhere in this window. The pain becomes more manageable, and mobility begins to improve in small but real ways. You may need less opioid medication by Day 5 or 6.
Swelling, however, peaks between Days 7 and 10. Your knee may look alarming, larger than before surgery and bruised in unexpected places. This is expected. Bruising can track down toward the calf and even to the foot due to gravity and the body's inflammatory process.
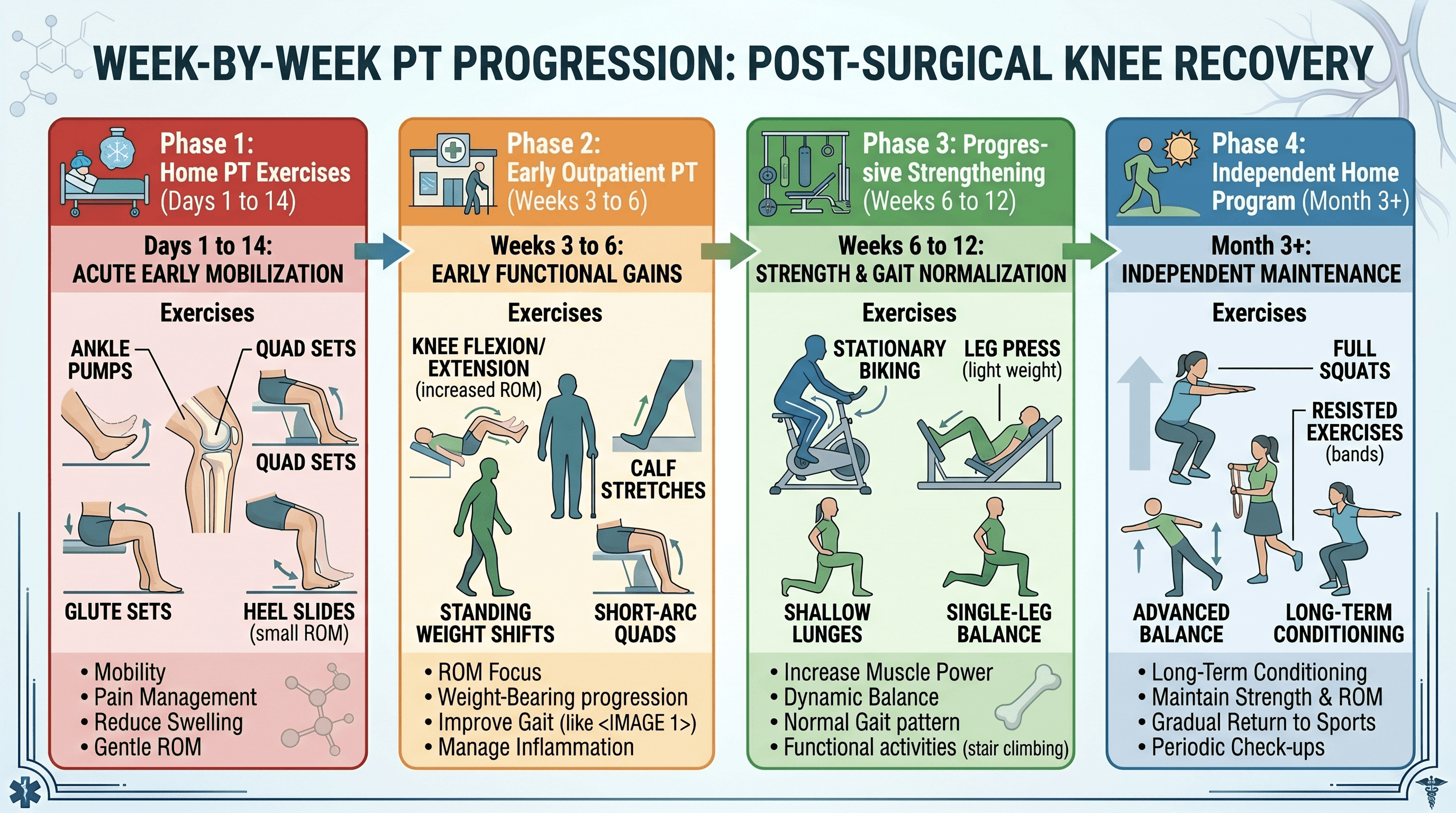
Physical therapy continues at home during this phase. Early exercises typically include heel slides (sliding the heel toward the body while lying on your back to increase knee flexion), quad sets (tightening the thigh muscle without moving the leg), ankle pumps (flexing and pointing the foot repeatedly), and seated knee extension (straightening the leg from a chair). These exercises are simple in description and genuinely difficult to do well when you're sore. Do them anyway. Consistency in the first two weeks sets up the entire trajectory of recovery.
A practical note that few guides mention: opioid pain medications cause constipation, and this can become its own significant discomfort by Days 4 to 7. A stool softener, such as docusate sodium, started on Day 1 and continued through the opioid course, combined with adequate hydration and fiber in your diet, helps prevent this problem before it starts.
Your first shower is a milestone typically cleared around Days 4 to 5, depending on your incision closure type. Ask your surgical team when the wound can safely get wet. Until then, sponge baths or a waterproof wound cover can help.
Days 6 to 10: Wound Healing and Finding a Sleep Routine
Incision care during this phase is straightforward but worth attending to carefully.
Your incision will be closed with staples, sutures, or surgical glue, depending on your surgeon's preference. Keep the area clean and dry until your care team clears you for showering with the wound exposed. Watch for early signs of infection: increasing redness spreading away from the incision, warmth that seems to be getting worse rather than better, any yellow or cloudy drainage, or a fever above 101°F. These warrant a call to your surgical team, not a wait-and-see approach.
Sleep disruption is one of the least-discussed and most genuinely difficult aspects of this recovery phase. Pain, positioning constraints, and the sedating-then-alerting effects of opioids can all fragment sleep significantly. The optimal sleep position for most patients is on the back with the knee slightly elevated on a pillow, not bent at a sharp angle. Sleeping on the stomach is not recommended in the early weeks. A wedge pillow or a rolled blanket under the lower leg can help find a supported position.
If night pain is waking you consistently, discuss timing of your pain medication with your care team. Taking a dose approximately 30 minutes before sleep can reduce nighttime disruptions.
Days 10 to 14: Suture Removal and Increased Independence
The first post-operative follow-up appointment with your surgical team typically happens around Days 10 to 14. This appointment serves several purposes: suture or staple removal, incision assessment, X-ray review of the implant positioning, and a conversation about your progress and next steps.
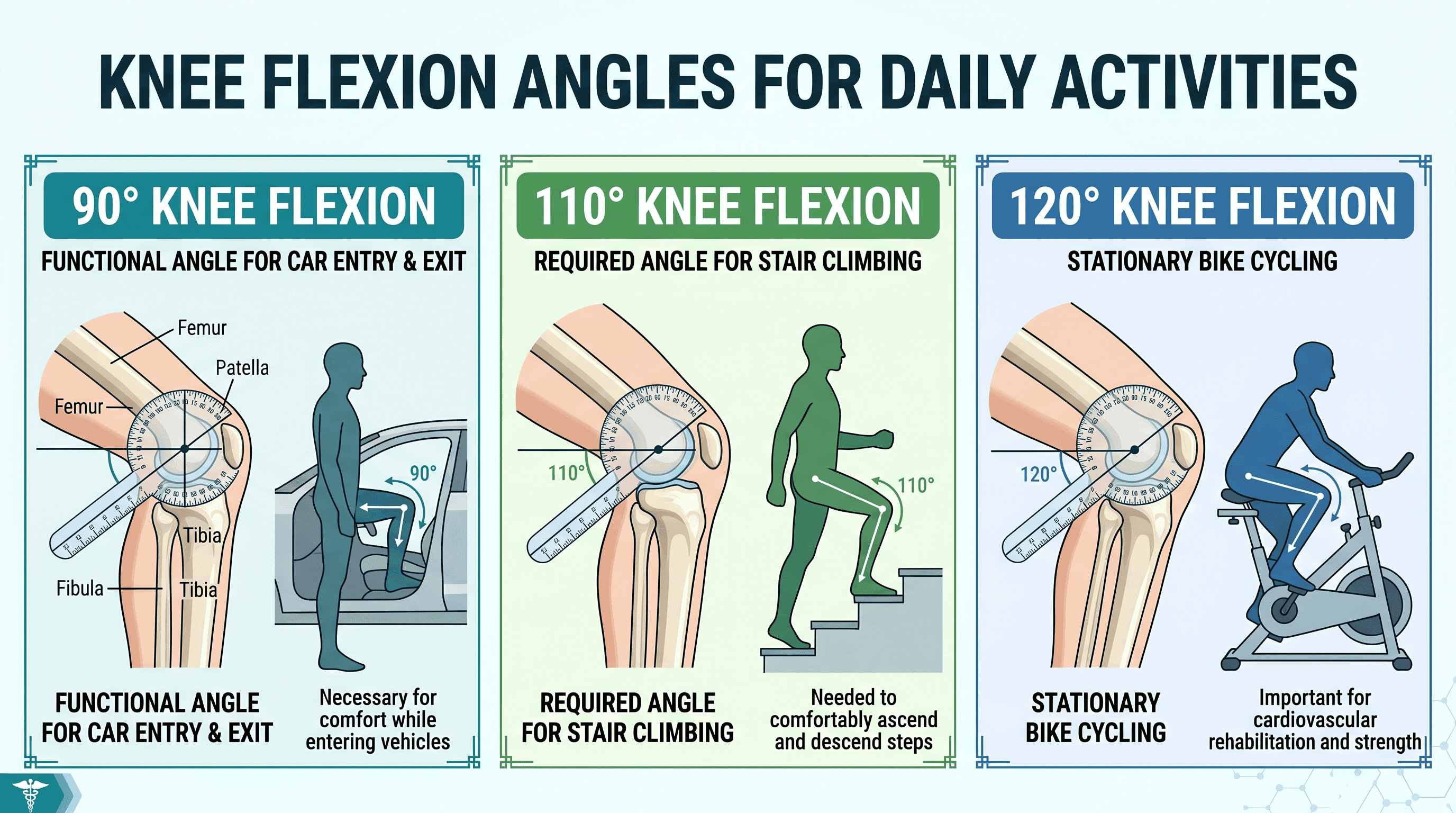
The clinical goal most surgeons aim for by approximately two weeks is achieving 90 degrees of knee flexion, meaning the knee bends to a right angle. This milestone matters because 90 degrees is roughly what is required to get in and out of a car, sit down in a standard chair, and navigate most everyday situations. If you have not yet reached 90 degrees, your PT will prioritize this aggressively in the coming sessions.
By Day 14, many patients have also transitioned from needing continuous assistance to managing short distances with a walker independently. The improvement from Day 3 to Day 14 is, for most patients, noticeable and motivating.
Weeks 3 to 4: Transitioning Walking Aids and Leaving the House
This is where many patients shift from a walker to a single-point cane, though the timing varies by individual. The transition to a cane is made when you can bear full weight on the operated leg without compensating significantly with your upper body or pelvis. Your PT will make this determination based on observation of your gait.
Use the cane on the opposite side from your operated knee, meaning if your right knee was replaced, carry the cane in your left hand. This is a biomechanical principle that offloads force from the healing joint.
Outpatient physical therapy typically begins around Weeks 3 to 4, supplementing or replacing home PT visits. Sessions usually occur two to three times per week. Outpatient PT introduces more demanding exercises aimed at rebuilding quadriceps strength, improving balance, and pushing range of motion further toward the 110 to 120 degree targets needed for full daily function.
A stationary bike is one of the best tools for gaining range of motion at this stage. The circular motion gently pushes the knee through its arc of motion in a low-impact, controlled way. Most patients can begin using a stationary bike at a low resistance setting sometime between Weeks 3 and 5, though a doctor can advise on timing for individual cases.
Leaving the house for short errands or walks becomes realistic in Weeks 3 to 4 for most patients. Start with flat surfaces and bring the cane. Outdoor terrain is less predictable than the hospital hallway, and protecting the operated knee from an unexpected stumble is worth the extra caution.
Weeks 4 to 6: Returning to Normal Daily Activities
By Week 4 to 6, most patients are managing the core activities of daily life with increasing confidence. Dressing, bathing, preparing light meals, and walking reasonable distances are all generally achievable.
Range-of-Motion Benchmarks: What the Numbers Mean
Orthopedic surgeons track knee flexion in degrees, and these numbers represent real-world function. Translating them:
Reaching 90 degrees means you can sit in a standard chair and get in and out of a car. Reaching 110 degrees means you can climb stairs in a typical foot-over-foot pattern rather than one step at a time. Reaching 120 degrees means you can ride a stationary bike with a normal pedaling motion and perform most recreational activities comfortably. The target at six weeks is typically between 90 and 110 degrees, with continued gains expected through Month 3 and beyond.
When Can You Drive After Knee Replacement?
Driving eligibility depends on several factors: which knee was operated on, whether your car is an automatic or manual transmission, and whether you are still taking opioid pain medication.
For a right knee replacement on an automatic transmission vehicle, most surgeons clear patients to drive between 4 and 6 weeks post-op, once the operated leg can perform an emergency stop reliably and you are fully off opioids. For a left knee replacement with an automatic transmission, some surgeons clear driving at 2 to 4 weeks since the left leg does not operate the primary driving pedals in an automatic. Manual transmission vehicles require both legs and therefore require the full clearance timeline regardless of which knee was replaced.
Do not drive while taking opioid pain medication, regardless of which knee was operated on. This is a patient safety requirement, not a suggestion. A doctor can advise on your specific clearance based on your progress.
Months 2 to 3: Reaching Maximum Daily Function
The three-month mark is a meaningful milestone in knee replacement recovery. By this point, Mayo Clinic notes that most patients are back to approximately 75% of their usual movement and daily functioning capacity.
Return-to-work timelines vary considerably by job type. Desk workers and those in sedentary roles can often return between Weeks 4 and 6. Jobs requiring prolonged standing, walking, or physical labor typically require 8 to 12 weeks or longer, with specific timing guided by the surgical team.
By Month 3, many patients have graduated from formal outpatient PT to an independent home exercise program. This transition is a sign of progress, not abandonment. The exercises your PT leaves you with are designed to continue building strength and flexibility through the remaining months of recovery.
Resuming sexual activity is a topic patients often hesitate to ask about. Most surgeons advise waiting approximately 4 to 6 weeks and recommend positions that do not place excessive torquing force on the operated knee. A doctor can advise on positioning specifics based on your individual recovery progress.
3 to 12 Months: The Long Tail of Recovery
This phase often surprises patients because the external markers of recovery, walking normally, managing stairs, returning to work, may be met while the knee itself still feels different from what they expected.
Residual swelling can persist for 3 to 6 months after surgery, and in some patients, warmth around the joint lingers even longer. This does not indicate a problem; it reflects the ongoing biological process of tissue remodeling around the implant. Mayo Clinic confirms that patients may still notice warmth and aching at the 9 to 12 week mark, with continued improvement over many months ahead.
Numbness along the outer (lateral) aspect of the incision is common and expected. Nerves cut during surgery regrow slowly, and some lateral numbness may persist for up to a year. For many patients it gradually resolves; for some, mild altered sensation in that area is permanent but not functionally limiting.
The question "why doesn't my knee feel normal yet?" is one of the most common questions at the 6-month mark, and the honest answer is: because full recovery genuinely takes up to a year. The implant integrates with bone, scar tissue matures, and the neuromuscular system relearns how to use the joint. Progress continues even when you stop noticing it day to day.
High-impact activities such as running, jumping, and contact sports are generally discouraged long-term to protect implant longevity. Low-impact activities including walking, cycling, swimming, golf, and hiking are widely recommended and encouraged, once fully recovered. An orthopedic surgeon can provide specific guidance based on implant type and individual recovery trajectory.
Pain Management After Knee Replacement: What's Normal, What's Not
Managing pain effectively in the early weeks is not about pushing through it. It's about staying ahead of it so you can do the movement and PT that actually drives recovery.
The multimodal approach most US hospitals now use combines acetaminophen on a scheduled basis, an anti-inflammatory medication if tolerated, and short-term opioid medication for breakthrough pain. This approach uses each drug's mechanism differently, allowing lower doses of each and reducing side effects compared to relying on opioids alone.
Opioids are typically tapered over approximately 4 to 5 weeks. Most patients no longer need them by the end of Week 5, though some are off them sooner. If you find you need opioids significantly beyond this window, discuss this with your surgical team as it can signal a pain management or recovery concern worth addressing.
Ice and elevation remain effective pain control tools throughout the first 6 to 8 weeks and are often underused. Applying ice for 15 to 20 minutes, three to four times daily, particularly after PT sessions, reduces inflammation and provides meaningful pain relief without medication side effects.
Expected surgical pain has a general character: it is present but responding to medication, broadly improving week over week, and localized to the operative site. Pain that is significantly worsening after the first week, that is accompanied by calf pain and leg swelling, or that comes with fever deserves prompt attention.
Physical Therapy: The Single Most Important Factor in Recovery
Physical therapy compliance predicts outcome more reliably than almost any other variable in knee replacement recovery. Research published in Acta Biomedica supports early mobilization and structured rehabilitation as cornerstones of successful recovery after total knee arthroplasty.
The reason PT matters so much is related to scar tissue. After surgery, the body's healing response produces fibrous tissue around the joint. This is normal. But if the knee is not moved through its range of motion consistently, that tissue can tighten and restrict flexion permanently. Scar tissue formation becomes problematic if PT is substantially skipped or delayed, particularly in the first 6 weeks.
Early exercises performed at home in the first two weeks include heel slides, quad sets, ankle pumps, and seated knee extensions. These exercises are the foundation on which outpatient PT builds. Outpatient sessions typically occur two to three times weekly and introduce progressive resistance, balance training, and functional movement patterns.
The home exercise program matters as much as the clinic sessions. A PT visit two or three times per week covers perhaps an hour and a half of structured movement. The other 22+ hours of the day still belong to you, and what you do with them shapes your outcome.
The Emotional Side of Recovery Nobody Talks About
Recovery from knee replacement surgery is physically demanding. But the emotional dimension, the parts no clinical checklist captures, deserves direct attention.
Research has documented a meaningful rate of mood-related symptoms following total knee arthroplasty. A formal diagnosis of post-operative depression occurs in a smaller subset of patients, but a substantially larger proportion report low mood, irritability, and emotional difficulty in the weeks following surgery. This is not weakness and it is not unusual.
Several factors converge to affect mood after surgery: anesthesia and opioids temporarily alter brain chemistry; sleep deprivation from pain and positioning constraints compounds this effect; the sudden loss of independence, particularly if you were active before surgery, can be genuinely disorienting; and the slow pace of early recovery can feel disproportionately frustrating when you expected to feel better.
Depression has been shown to correlate with worse functional outcomes after joint replacement, which is one reason addressing it matters practically, not just emotionally. If low mood, persistent anxiety, or withdrawal from normal activities persists beyond two to three weeks post-op, speaking with a primary care provider or mental health professional is a reasonable and appropriate step.
If you are supporting someone through this recovery, know that irritability and discouragement in Weeks 2 to 4 are often a normal response to a genuinely difficult situation, not a permanent state.
Why Am I So Tired After Knee Replacement? (And When Does It Improve?)
Post-operative fatigue is real, underappreciated, and has identifiable causes.
Anesthesia effects on alertness and energy typically persist for approximately one week. Opioid sedation adds to this through the tapering period, generally 3 to 5 weeks. The body's inflammatory response to surgery requires significant metabolic resources, which competes with energy available for everything else. Sleep disruption from pain and positioning compounds all of the above.
Most patients notice meaningful improvement in energy levels by Weeks 4 to 6, coinciding roughly with opioid tapering completion and the gradual normalization of sleep. Full energy recovery often tracks with overall functional recovery, improving progressively through Months 2 and 3.
Coping With Bad Days: Recovery Is Not a Straight Line
Recovery after knee replacement does not move forward at a steady gradient. Most patients experience a two-steps-forward, one-step-back pattern, particularly in Weeks 2 to 4.
A bad day, meaning a day with more pain, less range of motion, or more fatigue than the day before, does not reset the recovery clock. It is a fluctuation within an overall upward trend, not a reversal of progress. Inflammation levels vary day to day based on activity, sleep, stress, and hydration. This accounts for much of the variability patients experience.
Practical strategies for bad days: rest without catastrophizing (one rest day does not undo weeks of PT), ice and elevate proactively, do gentler exercises rather than skipping entirely, and contact your care team if a bad day is accompanied by new symptoms rather than just general soreness. Having one trusted person, a family member, friend, or care coordinator, who can provide calm reassurance during a hard stretch is genuinely helpful.
Nutrition and Sleep for Faster Recovery
What to Eat After Knee Replacement
Protein is the most consistently underemphasized nutrient in post-surgical recovery. The body uses protein to rebuild muscle and repair tissue, both of which are in active demand after knee replacement. Aiming for adequate daily protein intake, approximately 1.2 to 1.5 grams per kilogram of body weight, can support tissue repair during the active recovery phase. Good sources include eggs, poultry, fish, dairy, legumes, and protein-supplemented shakes.
Anti-inflammatory foods, primarily vegetables, fruits, whole grains, fatty fish, and olive oil, support the body's recovery process without the same level of evidence as protein but with well-established general health benefits. Processed foods, excess sugar, and alcohol are worth limiting during the recovery period.
Constipation prevention warrants its own attention. Opioid-induced constipation is very common in the first two weeks and can become genuinely uncomfortable. Strategies beyond the stool softener started at Day 1 include staying well hydrated (at least 6 to 8 glasses of water daily), incorporating fiber-rich foods like whole grains, beans, and fruits, and getting up and moving as tolerated, since even brief walking supports gut motility.
Sleep After Knee Replacement
The optimal sleep position for most patients in the first several weeks is on the back, with the knee slightly elevated on a firm pillow but not sharply bent. Sleeping on the stomach places unnecessary torque on the knee and is generally discouraged until healing is well advanced.
Practical sleep tips that make a difference: take pain medication 30 to 45 minutes before your intended bedtime if pain reliably disrupts your sleep; keep the room cool and dark to support sleep quality; avoid screens for 30 minutes before bed; and if opioid-related drowsiness makes you want to nap heavily during the day, try to limit naps to under 45 minutes to protect nighttime sleep architecture.
Warning Signs: When to Call Your Doctor
Most post-operative discomfort is expected and manageable. But certain symptoms require prompt attention, and knowing them in advance allows you to act without delay.
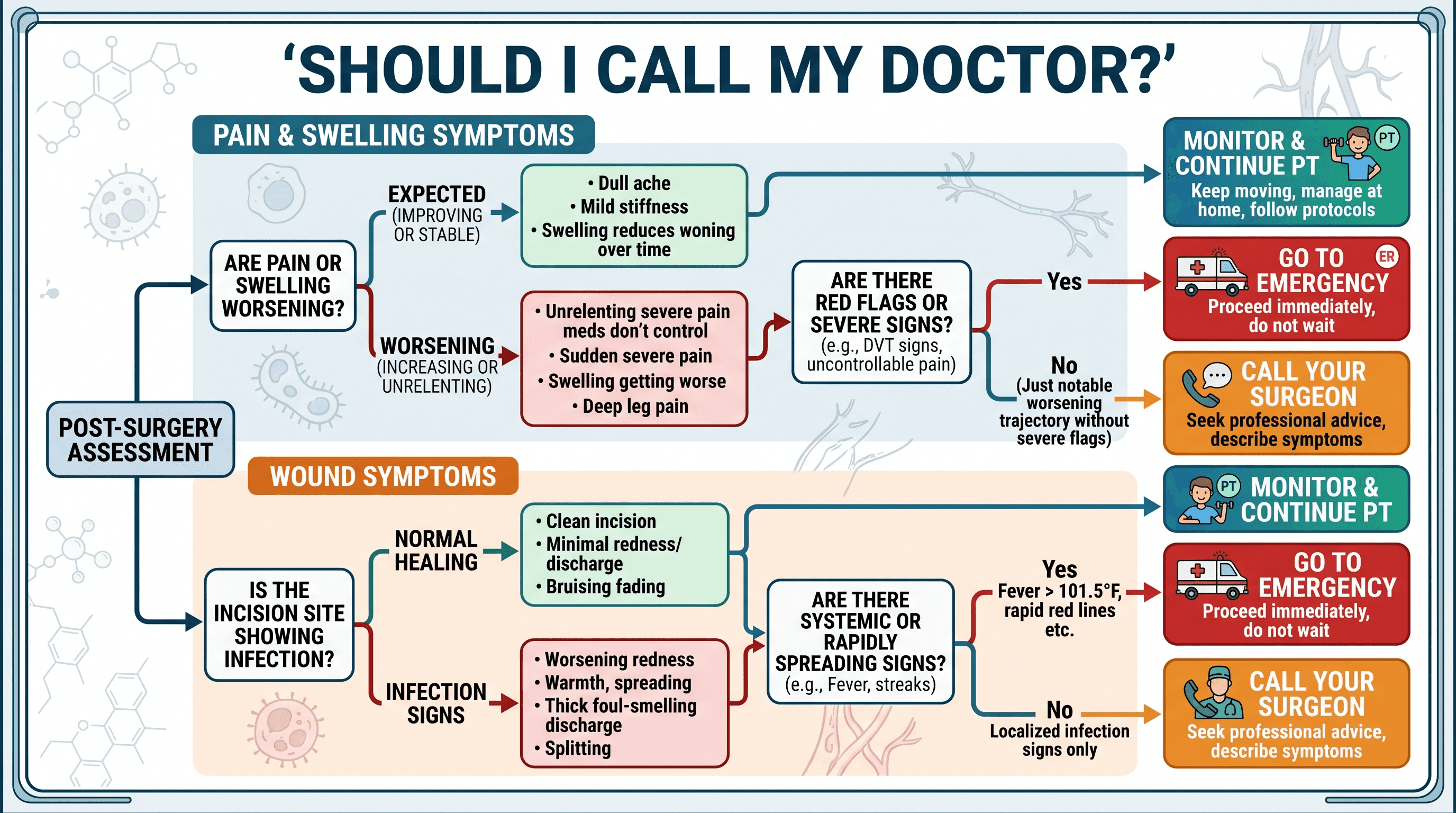
Deep vein thrombosis (DVT) signs include calf pain that feels like a deep cramping or tightness separate from knee soreness, swelling that is significantly more pronounced in one leg than the other, or new shortness of breath. These symptoms together or in combination warrant an immediate call to your care team or emergency services.
Infection signs include a fever above 101°F to 102°F, incision redness that is spreading or tracking beyond the incision margins, wound drainage that is yellow, cloudy, or foul-smelling, or increasing pain and warmth around the wound that is not improving with ice.
Concerning swelling is distinguished from expected swelling by its trajectory: expected swelling peaks around Days 7 to 10 and then gradually decreases. Swelling that is rapidly worsening after the first week, particularly with accompanying warmth and redness, deserves assessment.
Stiffness that is worsening rather than plateauing or improving after the first two weeks, despite consistent PT, is also worth discussing with your surgeon, as early intervention for restricted range of motion is far more effective than late intervention.
Recovery Milestone Checklist: Track Your Progress
This tracker gives you a concrete reference point so you know whether you are on a typical path.
By End of Week 1: Walking with a walker indoors over short distances; performing prescribed home exercises daily; pain managed with medication and ice; attending or completing initial PT sessions.
By End of Week 2: Showering independently (once wound cleared by care team); sutures or staples removed; approaching or reaching 90-degree knee flexion; walking more confidently with walker.
By End of Week 4: Walking short distances without walker or with cane only; outpatient PT underway 2 to 3 times per week; noticeably less opioid medication needed or off opioids entirely; able to manage most self-care tasks independently.
By Week 6: Most patients cleared to drive (right knee, automatic transmission); knee flexion approaching 110 degrees; sleeping more consistently; energy levels improving meaningfully.
By Month 3: Knee flexion reaching 120 degrees or beyond for many patients; returned to desk work and light daily activities; graduated or graduating from formal PT; walking distances increasing steadily.
By Month 6 to 12: Residual swelling continuing to resolve; lateral numbness improving (or stable and non-limiting); return to recreational activities cleared by surgeon; full functional recovery for most patients.
Directly answer the question "How do I know if my knee replacement is healing correctly?" by asking: Are you hitting these milestones within a reasonable range? Is pain trending down, even with setbacks? Is range of motion trending up? If yes to all three, you are healing as expected.
When to See a Doctor
If you notice warning signs from the section above, contact your care team promptly. But beyond acute warning signs, there are several less-urgent situations worth a conversation with your orthopedic team: pain that is not improving after Week 4 despite PT compliance; range of motion that has plateaued well below 90 degrees at the two-week mark; persistent mood symptoms affecting daily function; or any questions about returning to specific activities, sports, or work responsibilities.
For a referral to an orthopedic specialist or to find a physician who can guide your recovery plan, find a doctor through Momentary Lab and connect with a provider suited to your needs.
FAQ
How far should you walk each day after knee replacement?
In the first week, walking distances are short by necessity, typically just moving around the home and completing PT exercises. By Weeks 2 to 4, many patients can manage 10 to 15 minutes of walking two to three times daily. By Weeks 6 to 8, this often extends to 30-minute walks. The general principle is to increase distance gradually, monitoring for significant increases in pain or swelling after activity. If swelling is notably worse the morning after a longer walk, the distance was too much for that stage.
What are the hardest days after knee replacement?
For most patients, Days 2 and 3 are the hardest, as the nerve block wears off and pain reaches its peak before the medication regimen is fully established. The emotional difficulty of Weeks 2 to 3 also catches many patients off guard: this is the "week 3 slump" when the initial forward momentum stalls and improvement seems slower. Knowing both of these windows are coming and that they are temporary makes them substantially easier to navigate.
How many days should you rest after a knee replacement?
Rest and movement are both necessary, and the balance shifts over time. In the first two weeks, structured rest periods are important, but complete bed rest is counterproductive and increases clot risk. Movement is encouraged from Day 1. By Week 3, being on your feet for increasing periods is the goal. The concept of a "rest period" changes over recovery: early on it means elevating and icing between PT sessions; later it means taking rest days from vigorous PT while maintaining gentle daily movement.
What is the biggest complaint after knee replacement?
In the early weeks, the most common complaints are pain levels (particularly the Day 2 to 3 peak), sleep disruption, and constipation from pain medication. At 3 to 6 months, the most frequent concern is that the knee "still doesn't feel right" despite functional recovery. This is a normal feature of complete tissue healing, which takes up to a year, and not an indication that the surgery failed.
When does the fatigue improve after knee replacement?
Most patients notice a meaningful improvement in energy by Weeks 4 to 6, correlating with the end of the opioid taper and some normalization of sleep. Full energy recovery typically tracks with overall functional recovery and continues improving through Months 2 to 3.
Is depression after knee replacement surgery normal?
Low mood, irritability, and emotional difficulty are very common in the weeks following total knee arthroplasty. A formal diagnosis of depression occurs in a smaller subset of patients, but mood disruption driven by sleep deprivation, loss of independence, opioid effects, and inflammatory chemistry is a well-documented feature of this recovery. If mood symptoms are persistent or significantly interfering with daily life or PT participation, speaking with a healthcare provider is appropriate.
Need personalized guidance on your recovery plan? Momentary Lab's AI Healthcare Navigator can help you understand your options and find the right care resources for where you are in recovery.
References
- Cleveland Clinic: Knee Replacement (Arthroplasty) — Clinical overview of TKA procedure, recovery timeline, and complication risks.
- Mayo Clinic: Total Knee Replacement Surgery Patient Guide — Comprehensive patient education document covering recovery stages, wound care, mobility milestones, and discharge guidance.
- Lisi C et al., Acta Biomedica: Early Rehabilitation After Elective Total Knee Arthroplasty — Peer-reviewed evidence supporting early mobilization and structured PT in TKA recovery outcomes.



