
Knee pain has a way of becoming background noise. You adjust your route to avoid the stairs. You skip the walk with friends. You stop sitting on the floor. Then one day, the background noise is the loudest thing in the room, and a surgeon is showing you an X-ray that explains everything.
But an X-ray showing bone-on-bone contact does not automatically mean surgery is the next step. Knowing how to read your own symptoms, understanding what conservative care can and cannot do, and knowing the right questions to ask your orthopedic surgeon, those are the things that actually lead to a good outcome.
This guide is built for the decision phase. Not to push you toward surgery or away from it, but to give you a clear framework for making the call that fits your body and your life.
At a Glance
| Topic | Key Facts |
|---|---|
| Primary condition addressed | Knee osteoarthritis (most common reason for knee replacement) |
| Surgery type | Total knee arthroplasty (TKA) or partial knee replacement |
| Who is typically a candidate | Adults with severe OA whose pain persists despite 3 to 6 months of conservative care |
| When to consider surgery | When pain limits daily function, sleep, and quality of life |
| Modern implant lifespan | 20+ years with current prosthetic technology |
| Patient satisfaction rate | Approximately 87 to 90 percent report good to excellent outcomes |
| Recovery timeline | Walking same day; full recovery at 9 to 12 months |
What Knee Replacement Actually Does (And Does Not Do)
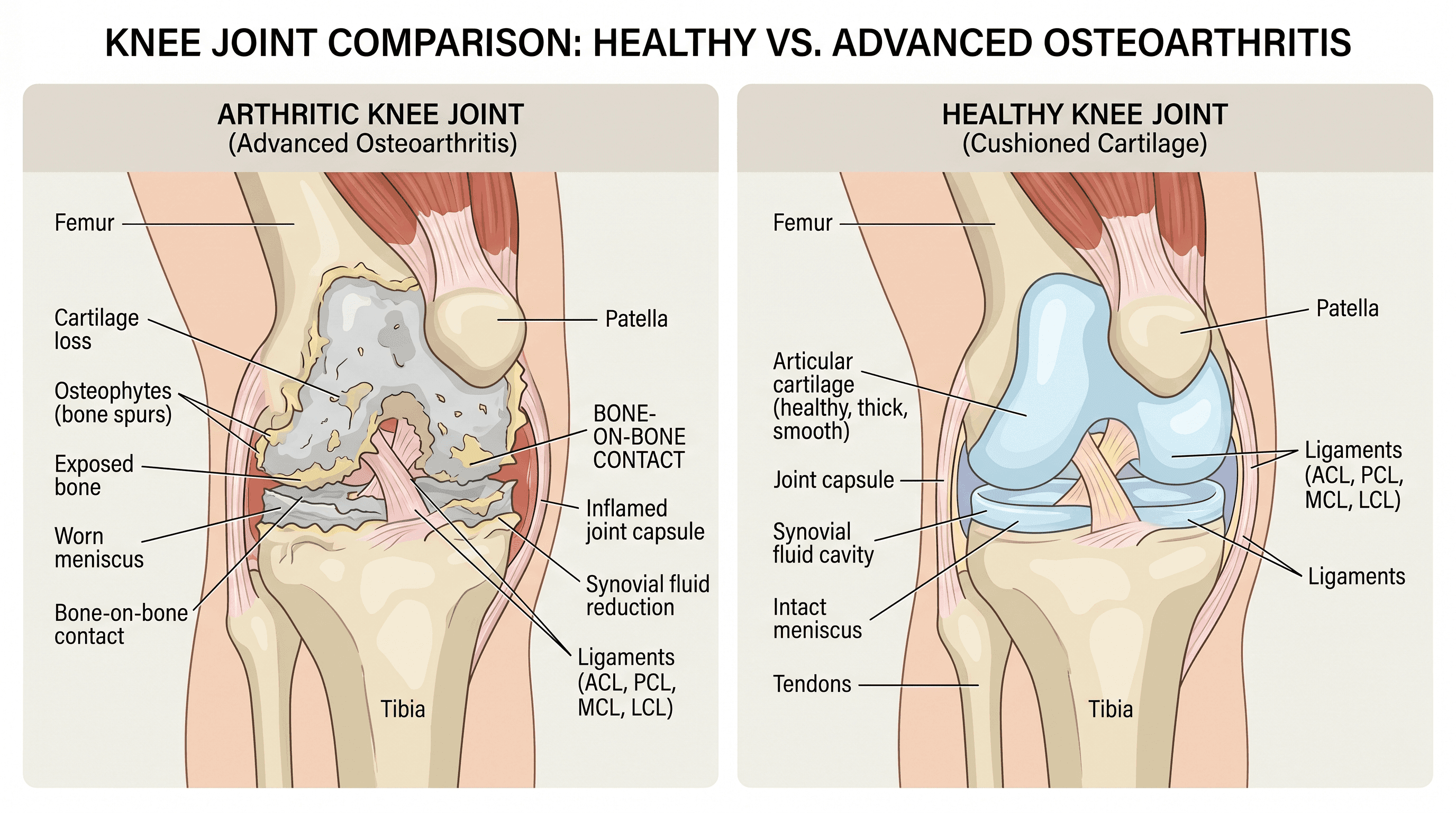
Knee replacement surgery resurfaces a damaged joint. It does not remove the knee or replace it with something mechanical from science fiction. The surgeon removes a thin layer of damaged cartilage and bone from the ends of the femur (thigh bone) and tibia (shin bone), then caps those surfaces with metal and plastic components that recreate smooth, pain-free movement.
What it does not do is restore a 25-year-old knee. Most patients gain significant pain relief, better mobility, and a return to daily activities. Return to high-impact sports like running or basketball is typically not the goal or the outcome. The procedure is designed to give you your life back, not to give you a new athletic career.
According to the Cleveland Clinic, knee replacement is one of the most successful procedures in orthopedic surgery, with the majority of patients reporting meaningful improvement in pain and function.
Signs You Need a Knee Replacement
No single symptom triggers a surgery recommendation. Orthopedic surgeons weigh a combination of clinical markers, imaging results, and how your symptoms affect daily life. These are the signals that, taken together, suggest conservative management has reached its limit.
Pain That Reorganizes Your Day
There is a meaningful difference between a knee that aches after a long walk and a knee that makes you plan every step of your day around avoiding pain. When a patient starts mentally routing around stairs before they even leave the house, when they are thinking about where the nearest bench is before they enter a store, that is the kind of pain that indicates advanced joint deterioration.
One clinicians sometimes call this the "dinner table test." If you are sitting at dinner and part of your attention is on your knee instead of the conversation, your pain has crossed from incidental to chronic. That level of persistent, intrusive pain is a meaningful clinical signal.
Night Pain That Disrupts Sleep
Rest pain is one of the clearest indicators that the knee has deteriorated beyond what conservative measures can address. When the joint aches at night without any activity triggering it, that reflects inflammation and structural damage that does not quiet down with rest.
According to Harvard Health, nighttime knee pain that consistently disrupts sleep is one of the factors orthopedic surgeons weigh heavily when assessing surgical readiness. Sleep disruption also compounds the experience of pain, lowering your threshold for discomfort and affecting overall health over time.
Loss of Ability to Fully Straighten or Bend the Knee
This is one of the most underrecognized warning signs, and it carries real urgency. When the knee loses its full range of motion, whether you cannot fully extend it straight or cannot bend it past a certain angle, that limitation may become permanent if the joint is left untreated too long.
After surgery, the amount of motion a patient recovers is partly determined by how much they had going in. Waiting until the knee has become stiff and contracted can mean that even a successful surgery does not restore full movement. If extension loss has developed, that warrants a prompt orthopedic evaluation.
Visible Swelling, Stiffness, and Joint Deformity
Swelling that is present most of the time, rather than just after activity, signals chronic inflammation that medication is no longer controlling. More advanced cases present with visible changes in leg alignment: a bowing outward of the knee (called varus deformity) or an inward lean (valgus, or "knock-knee"). These alignment changes reflect structural breakdown that affects how force is distributed across the joint.
The Mayo Clinic lists visible deformity and persistent swelling among the clinical criteria that typically indicate a patient is a strong surgical candidate.
Conservative Treatments Have Stopped Working
Surgery is always the last step, not the first. Before knee replacement is considered, most orthopedic guidelines recommend a meaningful trial of conservative care. That ladder typically includes physical therapy focused on quadriceps and hip strengthening, anti-inflammatory medications (NSAIDs), corticosteroid injections for acute flares, hyaluronic acid (viscosupplementation) injections, weight management, and assistive devices like bracing.
When a patient has worked through that ladder over several months and still cannot manage pain or maintain function, that is a clinical green light for the surgical conversation. The key distinction: failing conservative care means trying it adequately, not abandoning it after two weeks.
When You Should NOT Rush to Surgery
A reputable orthopedic surgeon will tell you this, and it is worth stating directly: not every candidate who meets the criteria above should schedule surgery immediately.
Several factors argue for delay or against surgery altogether. If pain is still manageable with conservative care and does not significantly limit daily activities, waiting is a reasonable and often recommended option. Patients with serious comorbidities including poorly controlled diabetes, recent cardiac events, or active infection near the knee carry higher surgical and anesthesia risks that must be addressed first.
Quadriceps strength matters significantly for recovery. Patients with very weak thigh muscles may benefit from a structured prehabilitation program before surgery. Open wounds, skin infections, or active skin conditions near the knee are absolute contraindications until resolved.
Perhaps most importantly, patients who are not prepared to commit to the rehabilitation process after surgery often see worse outcomes than those who delay until they are ready. Recovery from knee replacement requires consistent physical therapy for months. That is not a warning against surgery; it is a realistic expectation that helps people go in prepared.
The Timing Question: How Bad Does It Have to Be?
One of the most common questions people ask when searching for information on this topic is: "How bad does my knee have to be before surgery?" The answer is not a pain score or a specific X-ray finding. It is a combination of functional limitation, failed conservative care, and readiness.
What the research does clarify is that there are risks on both ends of the timing spectrum. Surgery too early (before conservative options are exhausted) exposes a patient to surgical risk without maximizing non-surgical options. Surgery too late can mean going into the procedure with severe muscle atrophy, fixed deformity, or loss of range of motion that limits what recovery can achieve.
Modern implants are designed to last 20 or more years. That longer lifespan has changed the conversation around younger patients. A 55-year-old with severe osteoarthritis is no longer automatically told to wait. The risk of a revision surgery decades later is weighed against years of continued pain and functional loss. Surgeons increasingly view age as one factor among many, not a threshold by itself.
Partial vs. Total Knee Replacement
About 90 percent of patients who undergo knee replacement surgery have damage affecting most or all of the knee joint, making total knee arthroplasty the appropriate choice. But for patients whose damage is confined to one compartment of the knee (the inner, outer, or front portion), a partial knee replacement is an option.
Partial knee replacement preserves more of the natural bone and tissue, which often means faster recovery and a more natural feel after surgery. The tradeoff is that if arthritis progresses in the other compartments, a conversion to total replacement may be needed later.
Your surgeon will assess which compartments are affected using imaging and physical examination. The right question to ask at your consultation is not simply "do I need surgery?" but "which parts of my knee are damaged, and does that affect which type of procedure makes sense for me?"
A 5-Question Self-Assessment Before Your Appointment
Before sitting down with an orthopedic surgeon, it helps to have clear answers to the questions they are likely to ask. Working through these in advance makes the consultation more productive.
How much does pain limit daily activities? Think specifically about walking distance, stair climbing, getting up from a chair, and dressing. If multiple activities are affected on most days, that is meaningful clinical data.
Does the pain wake you at night? Rest pain, as discussed, is one of the stronger indicators. Track frequency: how many nights per week does this happen?
What treatments have you tried, and for how long? Be specific: the name of the medication, the number of injections, how many weeks of physical therapy, and whether any of them provided meaningful relief and for how long.
Have you noticed visible changes in the knee? Swelling that does not resolve, changes in leg alignment, or a noticeable difference in how the knee looks compared to the other side are all worth mentioning.
Are you prepared to commit to rehabilitation? Honest self-reflection here is useful. Recovery from knee replacement is a multi-month process requiring daily exercises, multiple physical therapy appointments per week, and patience through a period of significant discomfort.
What Modern Knee Replacement Surgery Looks Like in 2025
The experience of having a knee replacement in 2025 is substantially different from what patients went through ten or even five years ago. Several advances have changed outcomes and recovery in meaningful ways.
Robotic-Assisted Surgery
Robotic-assisted knee replacement is now widely available at major orthopedic centers. The robot does not perform the surgery independently. It works as a precision guidance system that helps the surgeon position implants with greater accuracy than freehand technique alone allows. Research published in peer-reviewed journals has shown that robotic-assisted systems can improve component alignment, which affects how the implant feels during movement and how long it lasts.
The National Institutes of Health has published research examining the outcomes of robotic-assisted total knee arthroplasty and its effect on alignment and early functional results.
Outpatient Surgery and Faster Recovery Protocols
A significant shift in the last several years is the movement of knee replacement surgery toward outpatient settings. Many patients now go home the same day as their procedure rather than spending two to three nights in the hospital. This is made possible by advances in regional anesthesia (nerve blocks that reduce the need for heavy sedation), multimodal pain management that reduces opioid reliance, and enhanced recovery protocols that get patients walking within hours of surgery.
If you are evaluating surgeons, it is worth asking whether they perform outpatient knee replacement and what their specific enhanced recovery protocol involves.

What to Expect During Recovery
Recovery from knee replacement follows a reasonably predictable arc, though individual variation is real and influenced by age, fitness level, and how damaged the joint was before surgery.
Most patients stand and take a few steps with a walker on the day of surgery. The first two weeks involve significant pain, managed with a combination of medications, ice, and elevation, alongside daily exercises to prevent stiffness. Physical therapy begins within days and continues for several months.
By week six, most patients can walk with minimal or no assistive device and are working on building strength and improving range of motion. Between three and six months, the majority of daily activities (driving, household tasks, moderate walking) feel significantly more manageable. Full recovery, meaning the point where the new knee feels natural and function is maximized, typically takes nine to twelve months.
Between 87 and 90 percent of patients report good to excellent outcomes. The remaining 10 to 13 percent who report dissatisfaction most commonly cite unmet expectations rather than surgical failure. Patients who go into surgery with a realistic picture of what recovery involves, and what the procedure can and cannot deliver, consistently report better satisfaction.
How to Choose a Knee Replacement Surgeon
Zero of the top search results for this topic answer the question that naturally follows the decision to pursue surgery: how do you choose the right surgeon? These are the questions worth asking.
Is the surgeon board-certified in orthopedic surgery and fellowship-trained in joint replacement? Fellowship training means the surgeon completed additional focused training in joint replacement after their general orthopedic residency.
How many knee replacements does the surgeon perform per year? Volume matters. Research consistently shows that surgeons and hospitals with higher case volumes have better outcomes. A surgeon performing 150 or more knee replacements annually is considered high-volume in most literature.
Does the surgeon offer robotic-assisted surgery? Not every case benefits equally from robotic assistance, but a surgeon who has access to the technology and uses it regularly demonstrates investment in current technique.
What implant system does the surgeon use, and why? There is no single best implant for all patients. A surgeon who can explain their implant selection rationale based on your anatomy and activity level is more informative than one who uses the same system for every patient.
Where is the surgery performed? High-volume orthopedic hospitals and accredited ambulatory surgical centers have different profiles of risk and experience. Ask about infection rates and whether the facility has a dedicated joint replacement program.
To find a board-certified orthopedic surgeon in your area and compare credentials, search for a specialist through Momentary Lab's doctor finder to connect with qualified physicians near you.
Next Steps: Starting the Conversation With Your Doctor
If you have read through this guide and recognized several of the signs described, the right move is a formal orthopedic evaluation. Not a surgery date. An evaluation.
Bring a brief symptom log to the appointment: how long you have had significant pain, what activities it limits, what treatments you have tried and for how long, and whether night pain is present. Bring any imaging you already have, including X-rays or MRI reports.
Ask the surgeon to explain what your imaging shows in plain language, what options remain on the conservative side if any, and what surgical timing they recommend and why. A second opinion before committing to surgery is always appropriate and any surgeon worth consulting will support that.
The timeline belongs to you. This is a shared decision, and the goal is a knee that lets you live the life you want, not a surgery completed as quickly as possible.
For broader guidance on navigating health questions and finding the right care resources, the Momentary Lab AI Healthcare Navigator can help you explore conditions, understand your options, and prepare for medical appointments.
Frequently Asked Questions
How do doctors decide if you need a knee replacement? Orthopedic surgeons evaluate several factors together: the severity of symptoms (pain, stiffness, functional limitations), imaging findings showing cartilage loss or bone-on-bone contact, how the patient has responded to conservative treatments, and overall health status. No single test or finding triggers a surgery recommendation on its own. The decision is made by weighing all of those elements together with the patient's goals and readiness.
What are the first signs of needing a knee replacement? Early indicators include pain that limits daily activities like walking, stair climbing, or rising from a chair; stiffness that does not improve with rest or gentle movement; and swelling that persists through the day even without unusual activity. These signs alone do not mean surgery is necessary, but they warrant an orthopedic evaluation, particularly if they have been present for several months and conservative care has not helped.
Can you live with bone-on-bone knees without surgery? Some people manage bone-on-bone arthritis for extended periods using physical therapy, activity modification, assistive devices, and pain management. The feasibility depends heavily on the individual's pain tolerance, activity requirements, and overall health. The risk of waiting is that continued bone loss and joint deformity can make surgery more complex and limit how much function can be recovered afterward. A conversation with an orthopedic surgeon helps clarify whether continued conservative management is a realistic option for a specific case.
How bad does your knee have to be before surgery? There is no single pain score or X-ray grade that triggers a surgery recommendation. Surgeons look at whether pain significantly limits daily life, whether sleep is affected, whether visible deformity or alignment changes are present, and whether a meaningful course of conservative care (physical therapy, injections, medication) has been completed without adequate relief. The threshold is functional, not purely anatomical.
What is the difference between partial and total knee replacement? A partial knee replacement resurfaces only one compartment of the knee, preserving healthy bone and tissue in the other areas. A total knee replacement resurfaces the entire joint. Partial replacement typically allows faster recovery and a more natural-feeling result, but it is only appropriate when damage is confined to one compartment. About 90 percent of patients who need knee replacement require the total procedure.
Is there a minimum age for knee replacement surgery? There is no fixed minimum age. Surgeons weigh age as one factor among many. Younger patients may face the possibility of a revision surgery if they outlive their implant, though modern prosthetics are designed to last 20 or more years. Surgeons increasingly focus on the severity of disease, the failure of conservative care, and the impact on quality of life rather than age alone when making the recommendation.
References
- Cleveland Clinic: Knee Replacement — Clinical overview of knee replacement surgery, candidacy, and outcomes.
- Harvard Health: Is It the Right Time for a Knee Replacement? — Guidance on timing, including the significance of nighttime pain and functional limitation.
- Mayo Clinic: Knee Replacement — Clinical criteria for candidacy including visible deformity and persistent swelling.
- NIH/PMC: Robotic-Assisted Total Knee Arthroplasty — Peer-reviewed research on robotic-assisted knee replacement outcomes and component alignment.
- NIH/PMC: Outcomes and Patient Satisfaction in TKA — Research on patient satisfaction rates and factors influencing outcomes after total knee arthroplasty.



