
If you're staring at your knee brace at 11 PM, wondering whether tonight is the night you can finally leave it off, this guide is for you. The answer depends almost entirely on what type of meniscus surgery you had — and the gap between the two main procedures is wider than most patients expect.
At a Glance
| Topic | Key Facts |
|---|---|
| Primary keyword | When can I sleep without brace after meniscus surgery |
| Surgery type determines timeline | Meniscectomy vs. meniscus repair vs. root repair |
| Meniscectomy brace-free nights | Often within days to 2 weeks post-op |
| Meniscus repair brace-free nights | Typically 4 to 6 weeks in a locked brace |
| Root repair brace-free nights | Up to 6 weeks locked in full extension |
| Main risk of premature removal | Flexion contracture, scar tissue, possible revision surgery |
| Green light for brace removal | Surgeon or PT clearance, full passive extension, swelling controlled |
The Short Answer: It Depends on What Type of Surgery You Had
The type of meniscus surgery you had is the single biggest factor in determining when you can sleep without a brace. Two patients can have knee surgery on the same day and follow completely different protocols — one goes home with loose straps and freedom of motion, the other wears a rigid locked brace to bed for six weeks. Understanding which category fits your situation is the first step.
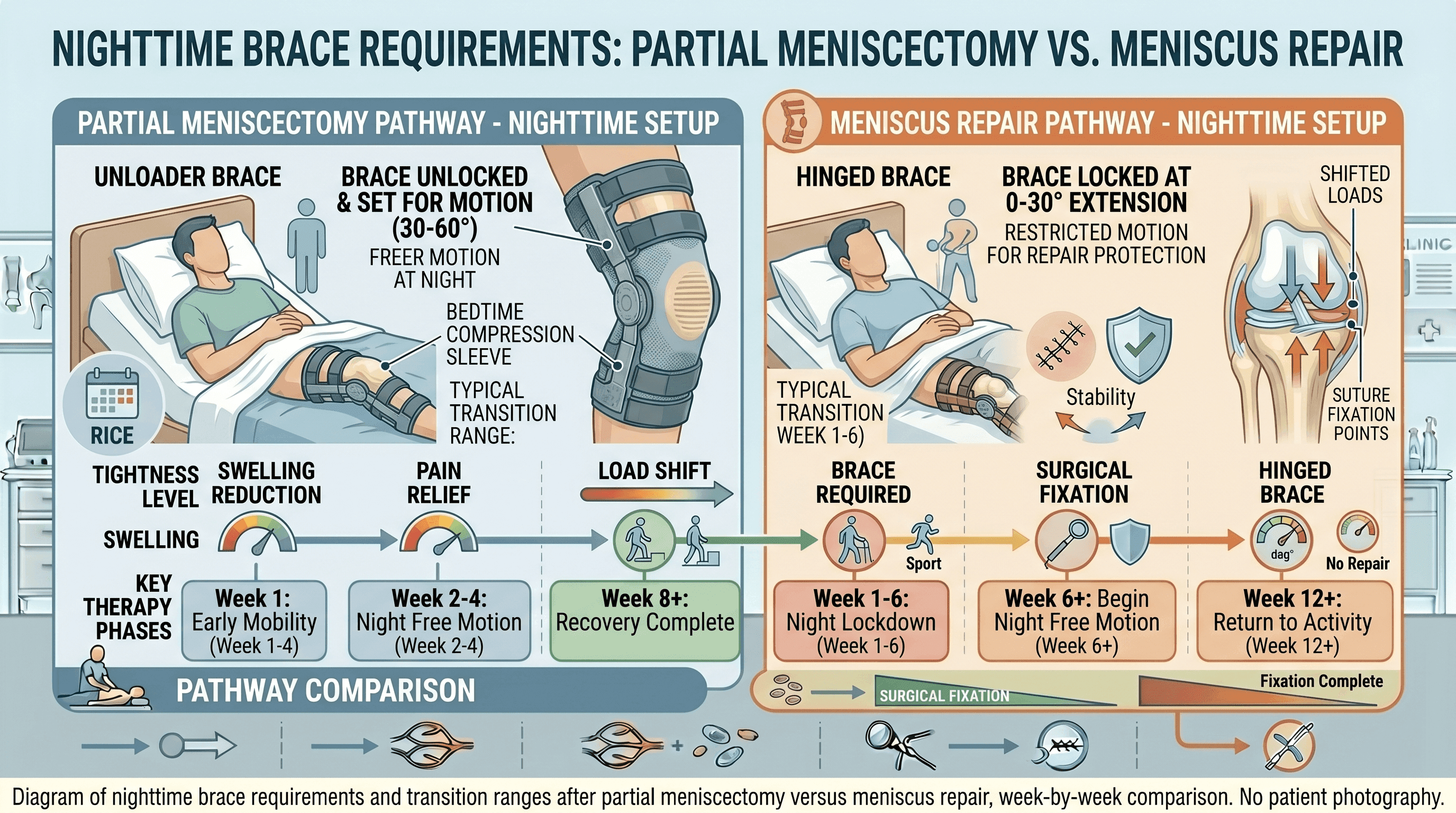
Partial Meniscectomy (Trimming)
A partial meniscectomy removes the damaged portion of the meniscus rather than repairing it. Because no sutures are placed and there is no healing tissue at risk of being stressed during sleep, post-op brace requirements are far more relaxed. Many surgeons do not require a nighttime brace at all after a meniscectomy, or they clear patients to sleep without one within days to two weeks — once swelling is under control and comfort allows. If a brace is prescribed, it is often for daytime stability rather than nighttime protection. Check with your surgeon, but this is generally the shorter, less restrictive path.
Standard Meniscus Repair (Suture Repair)
A meniscus repair uses sutures to reconnect torn cartilage tissue so that it can heal back together. Because the repair site is fragile during the early weeks, protecting it from unwanted motion during sleep is a real clinical priority. Most protocols following a standard meniscus repair require the brace to be locked in full extension (straight leg) during sleep for approximately four to six weeks. The exact duration varies by surgeon, tear location, and repair technique. This is the protocol followed by the majority of repair patients, and adhering to it is a meaningful part of avoiding re-tear.
Root Repair or Displaced Meniscus Repair
A meniscal root repair addresses tears at the attachment point where the meniscus anchors to the tibia bone. Root tears are treated as a more structurally significant injury because the meniscus loses its ability to distribute load across the knee when the root is detached. In plain terms: the repair is under higher mechanical stress, which means protection requirements are stricter. Root repair protocols commonly require the brace to be locked in full extension during sleep for the full six weeks post-op, and some surgeons extend nighttime bracing even longer. If your surgeon used the word "root repair" or "posterior horn repair," assume the more conservative timeline applies until told otherwise.
Why the Brace Matters While You Sleep
Most patients understand why a brace matters during the day — walking, weight-bearing, and bending are obvious risks. But sleep feels passive, which makes nighttime bracing feel excessive. It is not.
During sleep, involuntary movements happen constantly. Legs shift, knees flex, and the body rolls without any conscious input. For a repaired meniscus, an accidental deep bend or rotational twist in the first few weeks can place enough tension on fresh sutures to disrupt the repair site before the cartilage has fused. The cartilage has limited blood supply to begin with, which is why meniscal healing is slow and the repair environment must be carefully protected.
Beyond re-tear risk, there is a second concern: flexion contracture. A flexion contracture occurs when the knee loses the ability to fully straighten, often because scar tissue forms while the joint is held in a bent position during healing. Keeping the brace locked in extension during sleep actively prevents this by maintaining the joint in a neutral, elongated position throughout the night. According to Cleveland Clinic, keeping the brace on even at night is part of following surgeon directions to limit how much the knee bends after surgery — and those directions exist because the consequences of getting it wrong can include the need for additional procedures.
"As long as you follow your surgeon's directions for not bending your knee, your sleep position won't affect the healing process." — Dr. Joseph Tramer, Orthopaedic Surgeon, Cleveland Clinic
Week-by-Week Timeline: When Most Patients Transition Out of the Nighttime Brace
The table below reflects commonly reported protocol ranges across the three surgery types. Treat these as general reference points, not personal medical instructions. Your surgeon's specific guidance always takes precedence.
| Timeframe | Partial Meniscectomy | Standard Meniscus Repair | Root Repair |
|---|---|---|---|
| Week 0 to 2 | Brace optional or not required; comfort guides sleep | Brace locked in full extension at night | Brace locked in full extension at night |
| Week 2 to 4 | Most patients brace-free at night | Brace still locked in extension during sleep | Brace still locked in extension during sleep |
| Week 4 to 6 | No nighttime brace; focus on PT milestones | Surgeon may begin unlocking brace incrementally | Brace typically still locked; surgeon reassessment needed |
| Week 6 and beyond | Normal sleep positions resume | Nighttime brace often discontinued; soft sleeve may be used | Brace may continue or transition to soft sleeve per surgeon |
A 2024 survey of sports medicine orthopaedic surgeons published in the Orthopaedic Journal of Sports Medicine confirmed wide variation in post-repair rehabilitation protocols, which is why individualized guidance matters so much. A systematic review published in BMJ Open Sport and Exercise Medicine found broad variation across clinical rehabilitation studies, though early motion protocols were not associated with higher failure rates in select patient groups — still, bracing for sleep remained a common protective measure across most reviewed protocols.
Signs You Are Ready to Sleep Without the Brace
Knowing you are ready to remove the nighttime brace is not a self-assessment. It is a conversation with your surgeon or physical therapist, informed by specific clinical markers. That said, understanding what providers look for can help prepare for that conversation.
Full passive extension is one of the most important indicators. A healthcare provider can manually straighten your leg to the same degree as the opposite knee. If the repaired knee cannot fully extend passively, the brace may still be doing protective work. Active quadriceps control is another marker: the ability to perform a straight leg raise without the knee buckling or lagging. Swelling should be substantially reduced, since persistent swelling signals ongoing inflammation that protective immobilization may still be managing. And of course, formal clearance from your surgeon or PT is the final step — none of the above replaces a provider's direct assessment.
Think of this as a checklist to bring to your next appointment, rather than a checklist to work through on your own at home.
What If You Accidentally Slept Without Your Brace?
This happens more often than patients admit. You fell asleep on the couch, woke up at 3 AM without the brace on, or simply forgot after a long day. Before panicking, here is how to approach it.
First, assess for new symptoms. Do a quick check: is there sudden sharp pain along the joint line that was not there before? Has swelling dramatically increased overnight? Does the knee feel unstable when you try to straighten it? If the answer to any of those is yes, contact your surgeon's office when it opens — not the emergency room unless the pain is severe and unmanageable, but a same-day or next-day check is reasonable.
If you woke up, realized the brace was off, and feel roughly the same as you did before bed, one unbraced night is unlikely to constitute a repair failure on its own. A single incident of accidental removal early in recovery is worth reporting at your next appointment but does not automatically mean the repair is compromised. The repair is sutured in place; it does not unravel instantly. That said, this is one incident — patterns of skipping the brace are a different matter.
Going forward, a few practical strategies help: put the brace on before lying down for any rest, even a nap; use a pillow barrier on the side of the brace to reduce the chance of rolling onto the operative leg; and set an alarm reminder if drowsiness is making evening brace application easy to skip.
How to Sleep More Comfortably While Still Wearing the Brace
A locked knee brace is genuinely uncomfortable at night. That discomfort is real, and managing it directly affects sleep quality, which in turn affects recovery. Here are the most effective strategies.
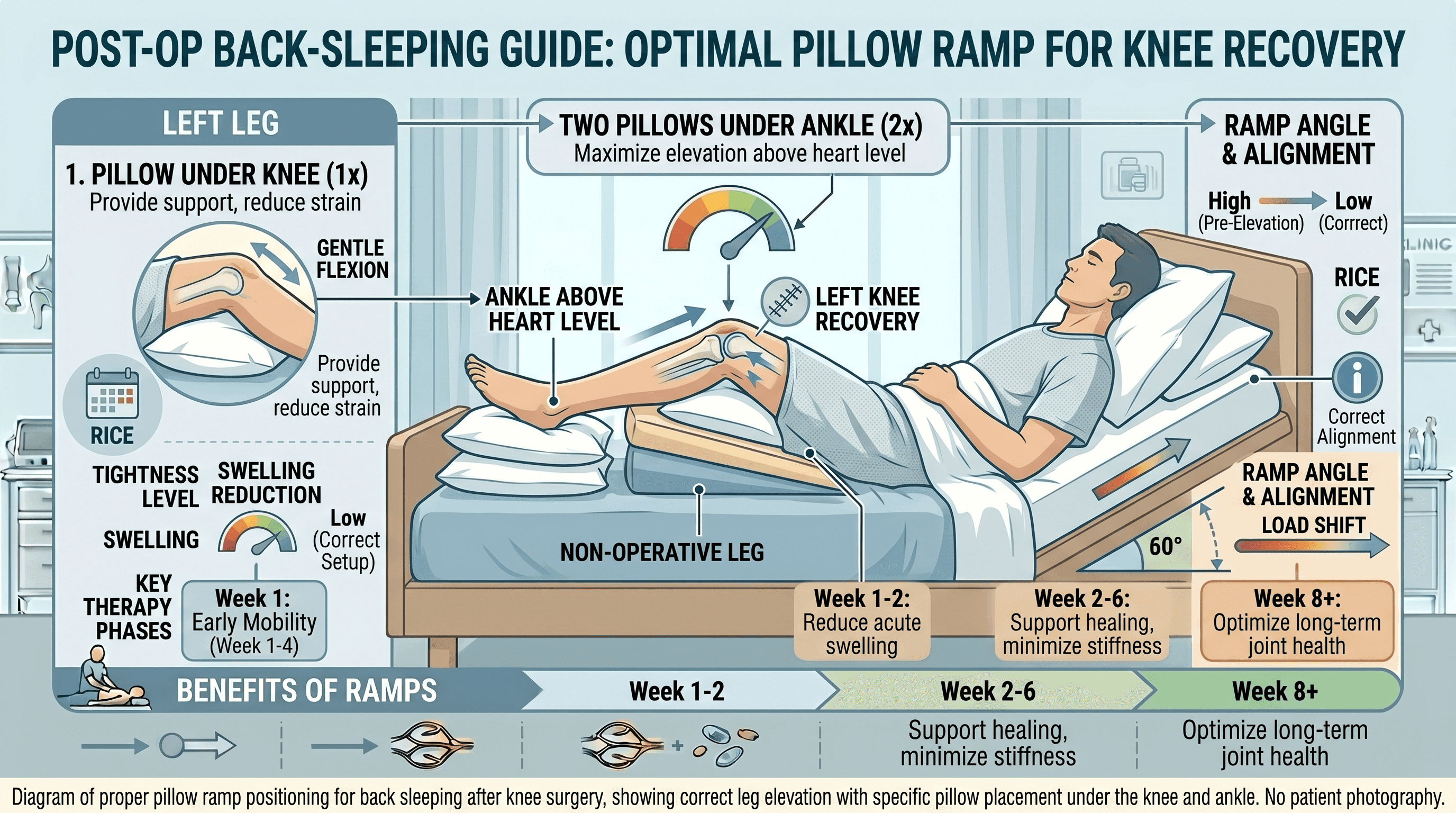
Back Sleeping Setup
Back sleeping is the most brace-friendly position, and it is the default recommendation from most post-op teams. Cleveland Clinic recommends creating a pillow ramp: one pillow positioned under the knee and two pillows stacked under the ankle. This lifts the leg above heart level, reducing overnight swelling by using gravity to improve circulation and reduce fluid accumulation in the knee joint. The angle should feel gentle, not sharply elevated.
Side Sleeping and When It Is Safe
Side sleeping is possible but requires more care. Lie on the non-operative side whenever possible. Place a pillow between the knees to prevent them from pressing together, which reduces both pain from contact and the risk of the brace torquing against the operative leg. Most surgeons clear side sleeping once the brace is unlocked and the patient has good leg control, typically around weeks four to six for repair patients. Ask your provider before making the switch.
Stomach sleeping is generally discouraged in the early weeks because it naturally encourages knee flexion, which works against the locked brace and can create uncomfortable pressure on the kneecap. Discuss with your surgeon if this is your preferred position.
Managing Brace Discomfort and Skin Irritation at Night
The padding inside a hinged knee brace compresses over time, and skin that is immobile against a hard plastic shell for hours develops irritation, pressure marks, and sometimes breakdown. Wearing a thin compression liner or a cotton sleeve under the brace creates a barrier that reduces friction significantly. Check strap tension before bed — the brace should be snug enough to stay in place but not so tight that it restricts circulation. Signs of over-tightening include numbness, tingling, or toes that feel cold and do not warm up within a few minutes of shifting position. Applying ice through a thin cloth before putting the brace on for the night can reduce pain and swelling enough to make the first hours of sleep substantially more comfortable.
The Transition Phase: Moving from a Locked Brace to a Soft Sleeve
Most repair patients do not go from a rigid locked brace directly to sleeping with nothing. There is typically an intermediate phase where the surgeon incrementally unlocks the brace to allow a progressively greater range of motion before full nighttime freedom is cleared.
In the first weeks, the brace is set to zero degrees, meaning no flexion permitted. As healing progresses and PT benchmarks are met, the surgeon or physical therapist may unlock it to allow up to 30 degrees, then 60 degrees, then 90 degrees — often in parallel with daytime rehabilitation goals. Nighttime restrictions tend to lag slightly behind daytime freedoms, because unsupervised sleep carries risks that daytime activity (where the patient is conscious and moving intentionally) does not.
Once the brace is fully unlocked and extension is maintained, the transition to a soft compression sleeve or no support for sleep typically follows. A compression sleeve provides mild joint warmth and proprioceptive feedback (the sense of where the joint is in space) without restricting motion. Many patients find this intermediate step reassuring before sleeping completely unsupported.
Beating the Morning Stiffness
Morning stiffness after a night in a locked straight brace is almost universal, and it can be alarming if you do not expect it. The knee spent eight hours in a single fixed position with minimal circulation through the joint. Synovial fluid, which lubricates the joint surfaces, distributes unevenly during prolonged immobility. The first attempts to move the knee can feel like bending a door hinge that has sat unused for months.
This is normal, and it usually resolves within 10 to 30 minutes of gentle movement. Before getting out of bed, try ankle pumps (repeatedly flexing and pointing the foot) to encourage circulation in the lower leg. Gentle quad sets, where you tighten the quadriceps muscle without moving the knee, help re-engage the muscle group that supports the joint. Once upright, a short walk with appropriate weight-bearing status helps distribute synovial fluid and reduce stiffness faster than staying seated.
If stiffness does not resolve within an hour or significantly worsens over time rather than improving, mention it at your next appointment. Progressive loss of morning extension is a signal worth investigating.
Warning Signs You Took the Brace Off Too Soon
Premature brace removal does not always announce itself immediately. Sometimes the joint feels fine the same night and the problem surfaces the following morning, or even a few days later.
Red flags that warrant a call to your surgeon include sudden sharp pain along the joint line (the sides of the knee where the meniscus sits) that was not present the previous day, a marked increase in morning swelling compared to recent days, a new sensation of the knee giving way or catching, and the inability to fully straighten the knee when it was extending normally the day before. Numbness or tingling in the lower leg or foot after brace removal should also prompt a call, as this can indicate circulatory or nerve compression issues related to brace fit rather than the joint itself.
One clear increase in pain after a single brace-free night does not automatically indicate repair failure, but it is reason to pause, replace the brace, and contact the surgical team for guidance. Do not wait through several days of increasing symptoms to report them.
When concerns arise, connecting with a qualified orthopaedic specialist promptly can prevent a small problem from becoming a larger one. Find a board-certified orthopaedic surgeon near you through Momentary Lab's physician directory to discuss your recovery questions and next steps.
Frequently Asked Questions
When can I stop sleeping with my brace after meniscus surgery?
The timeline depends on surgery type. After a partial meniscectomy, many patients are cleared within days to two weeks. After a standard meniscus repair, nighttime bracing in a locked position typically continues for four to six weeks. After a root repair, the timeline can extend to six weeks or longer. Formal clearance from your surgeon or physical therapist is required before discontinuing nighttime bracing.
How to sleep at night after meniscus surgery?
Back sleeping with a pillow ramp is the most recommended position: one pillow under the knee and two under the ankle to keep the leg elevated above heart level. Side sleeping on the non-operative side with a pillow between the knees is also acceptable for most patients. Timing pain medication one hour before bed, staying active during the day, and following good sleep hygiene practices all help improve sleep quality during recovery.
Can I drive two weeks after meniscus repair surgery?
Driving depends on which knee was operated on, whether you drive with automatic or manual transmission, whether you are still taking narcotic pain medications, and your surgeon's specific protocol. For right knee repairs, most surgeons require clearance before resuming driving because braking requires both speed and quadriceps control. Two weeks is often too early for repair patients, though meniscectomy patients may receive earlier clearance. A doctor can advise on individual cases based on recovery progress.
When can I fully bend my knee after meniscus surgery?
After a partial meniscectomy, range of motion generally returns within a few weeks as swelling resolves and physical therapy progresses. After a meniscus repair, full flexion is introduced gradually, often not until six to eight weeks or later, depending on the protocol. Attempting full flexion before the repair has healed can stress the suture site. Physical therapy benchmarks and surgeon clearance guide this progression.
Can I loosen the brace straps while I sleep?
Straps should be adjusted for comfort without compromising the brace's function. A brace that is too tight can restrict circulation; one that is too loose may shift during sleep and allow unwanted motion. The goal is snug but comfortable. If standard strap tension is consistently uncomfortable, contact the orthopaedic team — padding adjustments or brace modifications can often help.
Does sleeping without a brace too early damage the repair?
Possibly, yes. The meniscus sutures are under tension during the early weeks, and involuntary motion during sleep, particularly flexion beyond what the repair can tolerate, can disrupt healing. The larger clinical risk is flexion contracture: scar tissue forming with the knee in a bent position, which can permanently reduce full extension. One accidental brace-free night is worth monitoring but does not guarantee re-tear. A pattern of skipping the brace before clearance is significantly riskier.
If you have more questions about your knee recovery or want to explore your care options, Momentary Lab's health navigation platform can help connect you with the right information and resources for your situation.
References
-
Cleveland Clinic Health Essentials: How to Sleep After Meniscus Surgery — Clinical guidance on sleep positions, brace use, elevation, and pain management after meniscus surgery.
-
Cong T, et al. Current Practices for Rehabilitation After Meniscus Repair. Orthop J Sports Med, 2024. — Survey of AOSSM members documenting wide variation in post-repair rehabilitation protocols including bracing.
-
Spang RC III, et al. Rehabilitation following meniscal repair: a systematic review. BMJ Open Sport Exerc Med, 2018. — Systematic review of weight-bearing, range of motion, and immobilization protocols following meniscal repair.



