
Recovery from rotator cuff surgery looks different for a teacher than it does for almost any other profession. The standard advice, written for office workers or light-duty desk jobs, misses almost everything that makes classroom teaching physically demanding: the overhead whiteboard reach, the hallway crowd management, the constant lifting of laptops and stacks of student work, the sheer mental stamina required to be "on" for six hours straight while your body is still healing. This guide is written specifically for educators. It covers the honest recovery timeline, classroom accommodations worth requesting, legal protections available through FMLA and the ADA, and the exact functional milestones that signal a teacher is genuinely ready to walk back into a classroom.
At a Glance
| Topic | Key Facts |
|---|---|
| Modified return (sedentary duties) | As early as 2 to 6 weeks post-op with strict accommodations |
| Full classroom duties | Typically 4 to 6 months for small-to-medium tears |
| Dominant arm repair | Significantly extends grading, writing, and computer timelines |
| FMLA entitlement | Up to 12 weeks for eligible school district employees |
| ADA extension | Available after FMLA for larger tears requiring longer recovery |
| Best surgery timing | Start of summer break (June) for most academic-year teachers |
| Re-tear risk window | Highest in the first 24 weeks post-repair |
The Short Answer: When Can You Get Back to Your Students?
Most teachers can consider a modified return to classroom duties somewhere between two and six weeks after rotator cuff surgery, but "modified" carries a lot of weight in that sentence. Full, unrestricted classroom duty, including whiteboard writing, lab supervision, physical student management, and carrying materials, typically takes four to six months for small-to-medium tears and can extend to twelve months for large or massive repairs. The Haunschild et al. 2021 systematic review and meta-analysis published in the American Journal of Sports Medicine found that the overall mean time to return to work across occupations was approximately 4.4 months, with manual and physically demanding roles returning significantly later than sedentary ones. Teachers occupy a middle ground that most generic timelines do not account for.
The realistic picture is this: a light-duty, seated, voice-led return is possible relatively early in recovery if a school and surgeon agree to the accommodation plan. A full return to all classroom duties is a longer road, and trying to shortcut it carries a genuine re-tear risk during the critical tendon-healing window.
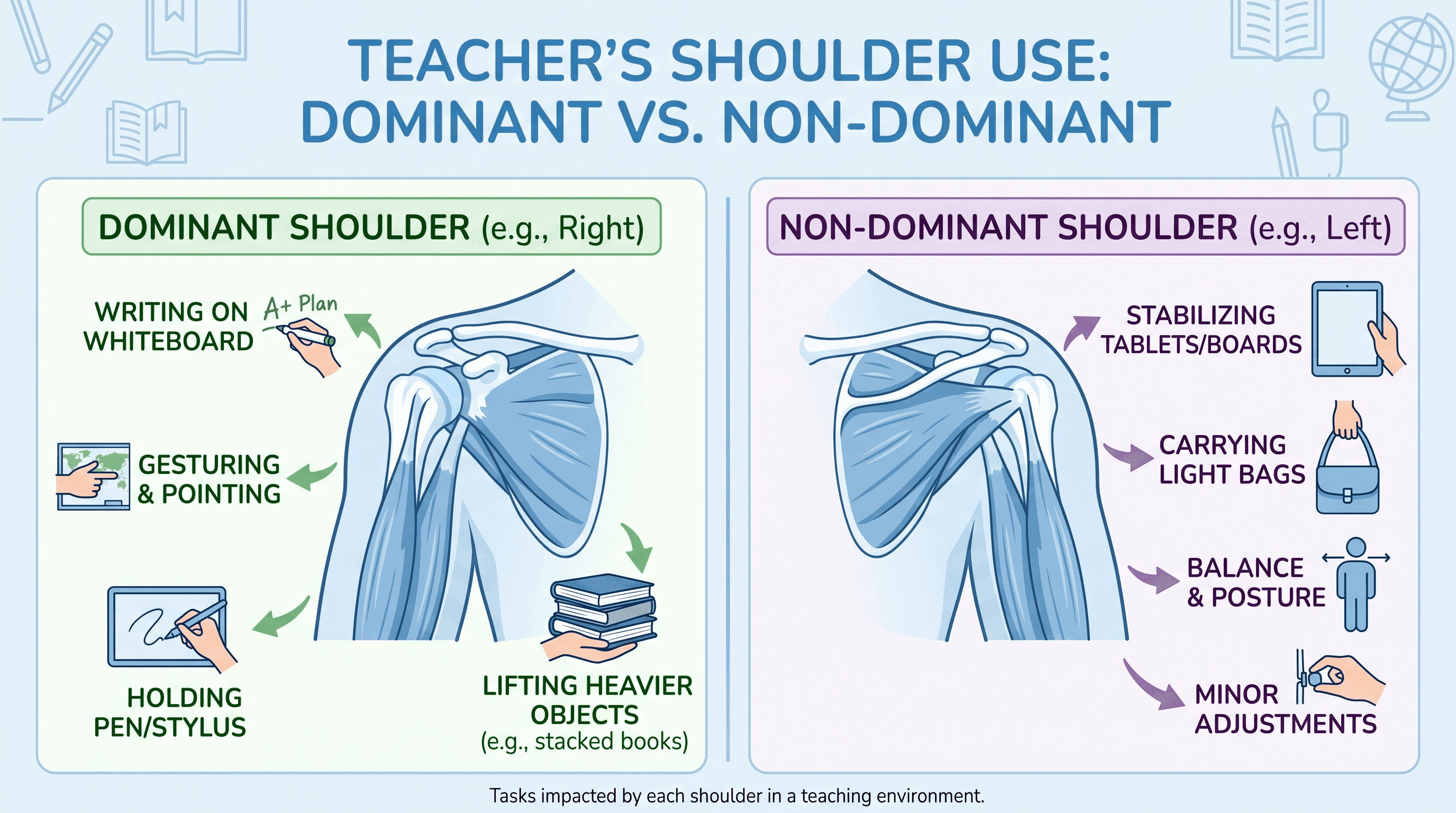
The Dominant vs. Non-Dominant Arm Dilemma
Which shoulder was repaired changes the classroom calculus significantly.
When the non-dominant arm is repaired, the functional impact on core teaching tasks is manageable early in recovery. Writing on a whiteboard, grading papers, and using a keyboard remain intact. The main challenges become carrying and lifting with the non-dominant side, managing hallway supervision safely, and driving restrictions in the first four to six weeks.
When the dominant arm is repaired, the job becomes far harder. Whiteboard writing, handwriting comments on student papers, mousing a computer, and even signing hall passes require adaptation from day one. Teachers repairing their dominant arm typically benefit from planning digital alternatives before surgery: voice-to-text software for grading feedback, a projector or smartboard replacing all physical whiteboard work, and a seating arrangement that eliminates the need to reach or lift. A return to full grading and handwriting-intensive work generally aligns with the broader clinical recovery timeline, around four to six months post-op for most tears, depending on repair size and individual healing.
The Hidden Physical Demands of Teaching
Teaching is not a desk job, and its physical demands are consistently underestimated in standard return-to-work guidance.
A classroom teacher's workday involves repeated overhead arm movement for whiteboard use, carrying stacks of papers, textbooks, and laptop bags that can weigh between 10 and 30 pounds, bending to assist students at desks, physical redirection or steadying of students in special education or early childhood settings, hallway and cafeteria supervision in crowded spaces where shoulder contact is a real risk, and prolonged standing that increases whole-body fatigue while the shoulder is still healing. Physical education teachers add an entirely separate layer: demonstrating movements, spotting students, managing equipment, and in some settings, physically assisting students through activities.
Beyond the mechanics, there is the cognitive and emotional load. Managing a classroom while managing pain, restricted range of motion, and the anxiety of protecting a healing tendon is genuinely exhausting in a way that does not show up on a standard restrictions form. Fatigue during recovery is real and often underreported; it compounds the physical risk and should be factored into any return-to-work plan alongside purely physical limitations.
What Happens to Your Shoulder During Rotator Cuff Surgery
Rotator cuff repair involves reattaching a torn tendon, usually the supraspinatus, back to the head of the humerus using suture anchors. The tendon does not "heal" the way a skin cut does. Instead, the repair site undergoes a biological process called tendon-to-bone healing, which progresses through an inflammatory phase, a proliferative phase, and a remodeling phase over many months. According to Mayo Clinic, the repaired tendon remains mechanically vulnerable for the first four to six months while this biological integration is ongoing. This is the same window in which most teachers are eager to return to full duties, and it is the window in which re-tears are most likely to occur if the shoulder is overloaded.
Tear size matters significantly. Small and medium tears (less than 3 cm) heal more predictably and allow earlier functional recovery than large tears (3 to 5 cm) or massive tears (greater than 5 cm), which carry higher re-tear rates and longer recovery timelines regardless of occupation.
The Realistic Recovery Timeline for Teachers
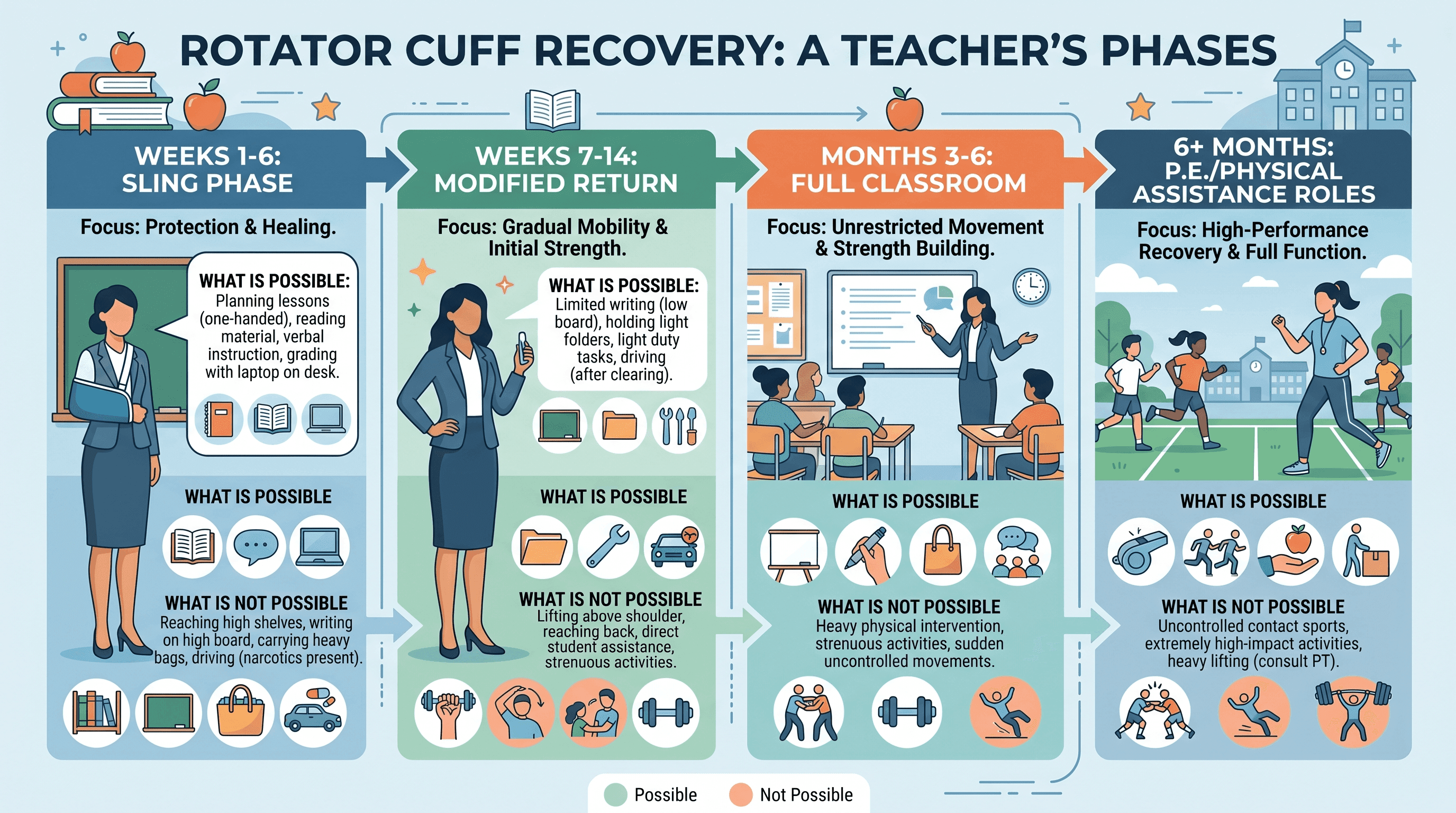
Recovery unfolds in phases, and the phase you are in determines what is and is not safe to attempt at school.
Weeks 1 to 6: What You Realistically Can and Cannot Do
The shoulder is in a sling during this phase, and the primary goal is protecting the repair, not rehabilitating it. For teachers, most classroom duties are not feasible during this window. Writing on a whiteboard, carrying anything heavier than a light folder, driving (especially with a dominant arm repair), and managing student physical contact are all outside safe limits. A teacher who returns to any in-person role during weeks one through six should be doing so in a fully supported capacity: seated, no sling-side lifting, no hallway or cafeteria duty, and with a substitute or paraprofessional handling all physical classroom management.
Many teachers on FMLA choose to use this window entirely for recovery and to avoid the real risk of a re-injury from an early classroom misjudgment.
Weeks 7 to 14: The Window Where Partial Return Becomes Possible
Physical therapy becomes more active during this phase, and some functional capacity returns. A teacher repairing a small-to-medium tear may find that a structured partial return, with smartboard use replacing whiteboard writing, a rolling cart replacing bag-carrying, and no lab or physical supervision duties, is genuinely manageable. The Haunschild et al. meta-analysis found that return to work rates improved steadily from the two-month mark onward for non-manual occupational groups. That said, a doctor's formal clearance for modified duty is a prerequisite, not a suggestion.
Months 3 to 6 and Beyond: Full Classroom Duties and P.E. Teachers
For standard classroom teachers with small-to-medium tears, months three through six typically mark the graduation toward full duties. Range of motion improves substantially, strength begins returning, and the re-attach site becomes progressively more stable. According to Cleveland Clinic, most patients regain full function somewhere between four and six months post-surgery, though individual variation is significant.
Physical education teachers are in a separate category. P.E. instructors must be cleared for demonstrating movements, managing sports equipment, physically spotting students, and, in some settings, intervening in physical altercations. Full clearance for P.E. teaching duties typically aligns with the later end of the six-month timeline or beyond for large tears, and should always follow an explicit functional assessment rather than a calendar date.
Special education teachers and early childhood educators who provide physical assistance to students face similar timelines to P.E. teachers, because the physical demands of their setting are broadly equivalent to light manual labor, not sedentary office work.
Surviving the Sling Phase at School
If a teacher returns during the sling phase for any reason, including performing limited duties from a desk, the school environment itself becomes a hazard to manage.
Crowded hallways during class changes are the single highest-risk environment for a healing shoulder. A single inadvertent bump from a student, a door swinging open, or a backpack collision can put direct force on a repaired tendon that has no margin for unexpected load. Teachers in slings who are on campus should request a hallway plan that routes them away from high-traffic transitions and assigns hallway duty to other staff entirely.
Classroom management of energetic students, particularly in elementary school or middle school settings, carries a similar risk. Reflexive reaching, grabbing, or bracing movements are essentially involuntary, and they can happen faster than conscious thought during a student incident. A written agreement with administration documenting that the teacher is not responsible for physical student management during recovery is worth having on record.
Morning routine and dressing adaptations also warrant mention. Many teachers underestimate how much energy goes into getting dressed and commuting before the school day begins. Fatigue accumulates early, and arriving at school already tired from the physical effort of self-care in a sling is a legitimate factor in recovery planning.
Crucial Classroom Modifications and Accommodations
The accommodations below are not about making things easier. They are about making a structured return medically sound while protecting both the teacher and the repair.
A Sample Accommodation Request Checklist for Teachers
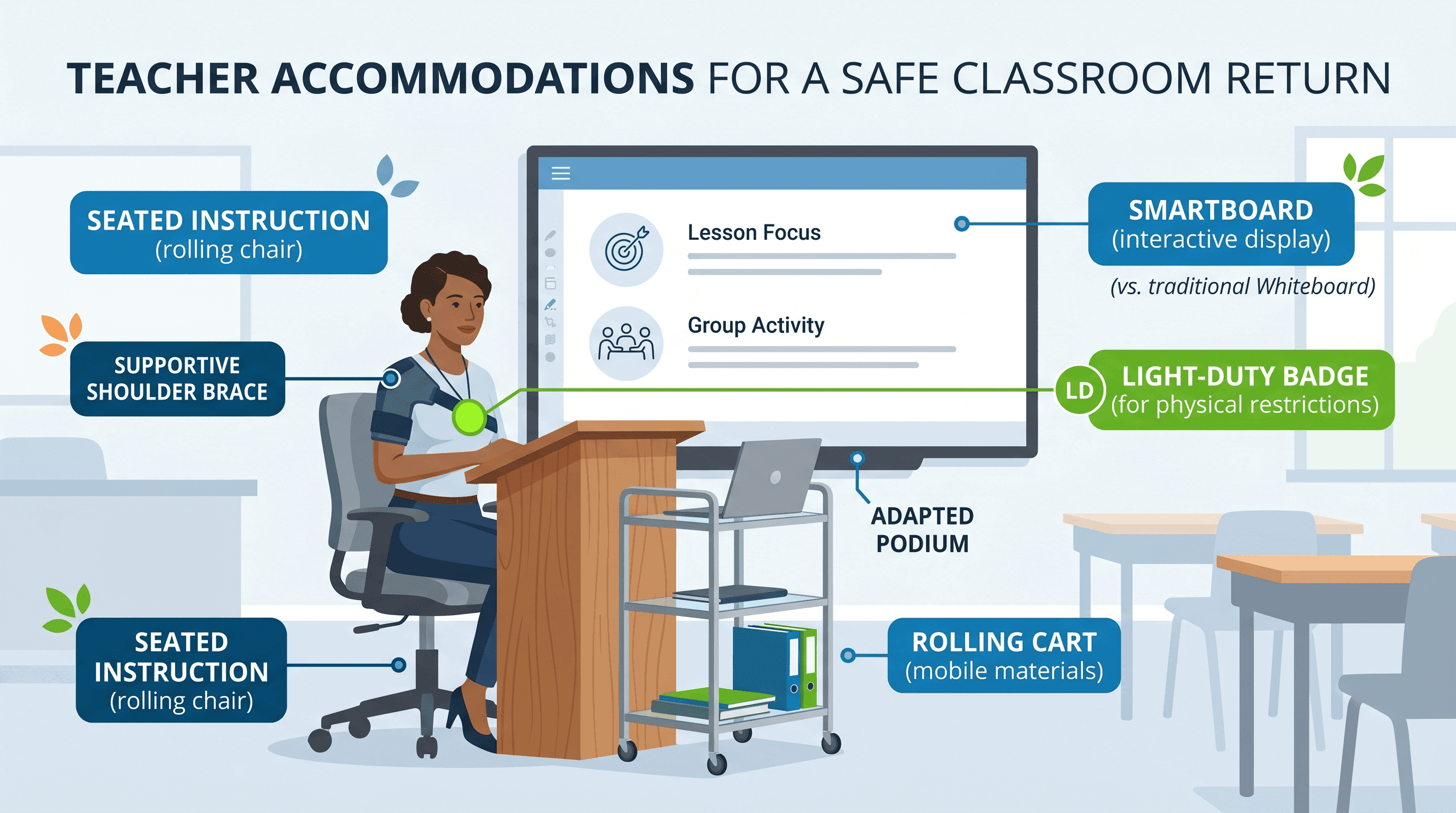
When requesting accommodations from a principal or HR coordinator, a written list submitted alongside the surgeon's restrictions note is far more effective than a verbal conversation. The following modifications are reasonable to request based on the physical demands of classroom teaching during shoulder recovery.
A smartboard, projector, or document camera replacing all overhead whiteboard writing removes the most biomechanically risky repetitive movement from the classroom day. A rolling cart or assigned student helper for all material transport eliminates the carrying loads that most districts do not formally classify as a job requirement. Removal from hallway duty, cafeteria supervision, and lab setup during the restricted period is a reasonable functional adjustment. A height-adjustable podium or standing desk with armrest support reduces the static load on the recovering shoulder during instruction. Formal documentation that physical student management, including restraint, redirection, or physical assistance, is reassigned during recovery is both a safety measure and a legal protection. In secondary and higher-grade settings, a student proctor or paraprofessional assigned during test administration can handle distribution and collection tasks.
Sample language for the request: "Per my surgeon's postoperative restrictions dated [date], I am unable to perform overhead reaching, carry loads exceeding [X] pounds, or provide physical student management through [estimated clearance date]. I am requesting the following modifications to allow a safe, modified return to instructional duties..."
What Your School Is and Is Not Legally Required to Provide
Under the Americans with Disabilities Act, employers, including school districts, are required to provide reasonable accommodations for employees with qualifying conditions unless doing so creates an undue hardship. A rotator cuff repair with documented restrictions generally qualifies. According to the ADA National Network, "reasonable accommodation" does not mean eliminating all physical job functions permanently, but it does require the employer to engage in an interactive process to identify what modifications will allow the employee to perform essential job functions.
What schools are not required to do: eliminate the teaching function entirely, permanently reassign duties, or create an entirely new position. What they are required to do: have a good-faith conversation about what modifications are feasible and document that process.
Your Legal Rights: FMLA, ADA, and Teacher-Specific Protections
This section covers ground that no generic rotator cuff article addresses, and it may be the most valuable section in this entire guide for educators.
FMLA for Teachers: What Is Covered and for How Long
The Family and Medical Leave Act entitles eligible employees to up to 12 weeks of unpaid, job-protected leave per year for a serious health condition, including rotator cuff surgery and recovery. According to the U.S. Department of Labor, covered employers include any public agency (which includes public school districts regardless of size) and private employers with 50 or more employees. Most public school teachers are automatically covered.
FMLA leave does not have to be taken all at once. Intermittent FMLA, taken in days or part-days, is available and particularly useful for teachers managing physical therapy appointments, post-op follow-ups, or recovery setbacks during a modified return.
FMLA is unpaid unless the employer requires, or the employee chooses, to substitute accrued paid leave, such as sick days or personal days, concurrently.
When FMLA Runs Out: ADA Accommodations and Extended Leave
For teachers with large or massive tears whose recovery extends beyond 12 weeks, the ADA provides a secondary framework. Leave beyond FMLA can qualify as a reasonable accommodation under the ADA, according to the ADA National Network, as long as the leave is finite and the employee can return to the essential functions of the job after a defined period. This is not automatic. The teacher must request it, provide medical documentation of the expected return date, and engage in the employer's interactive process.
Union Protections and Sick Leave Banks (NEA/AFT Members)
Teachers who are members of National Education Association (NEA) or American Federation of Teachers (AFT) affiliated locals may have additional protections through collective bargaining agreements that go beyond federal minimums. Many district contracts include sick leave banks, which allow teachers facing extended medical leave to borrow sick days from a collectively funded pool. Some agreements also include long-term disability provisions and return-to-work protocols with stronger accommodation language than the ADA baseline. Teachers should review their local contract and consult their union representative before finalizing any leave plan.
Pay, Insurance, and Financial Planning During Your Leave
The financial impact of rotator cuff leave is real, and it deserves honest attention.
Using Sick Leave and Disability Benefits During Recovery
FMLA leave is job-protected but not automatically paid. Most teachers will use accrued sick days first, running them concurrently with FMLA. Once sick days are exhausted, short-term disability insurance becomes relevant. Many school districts offer short-term disability coverage as part of their benefits package, typically replacing 60% of salary for a defined benefit period. Teachers should verify their policy terms, including the elimination period (the waiting days before benefits begin) and the maximum benefit duration, before surgery if possible.
Workers' Compensation: Was Your Injury Job-Related?
If the rotator cuff injury occurred at school, whether from breaking up a student altercation, a fall on school property, or repetitive overhead demands that can be documented as occupational, a workers' compensation claim may apply. Workers' comp, when approved, covers medical treatment and a portion of lost wages without drawing against personal sick leave. The key threshold is establishing a causal connection between the job and the injury. Teachers who were injured during a student intervention, for example, have a documented incident that typically satisfies this requirement. A doctor advising on individual circumstances is the right starting point for any compensation-related question.
If teachers want help finding the right physician for post-op clearance or return-to-work documentation, finding a qualified orthopedic specialist through a verified provider directory is a practical first step.
Strategic Planning: When Is the Best Time to Schedule Your Surgery?
Timing is the one variable teachers have genuine control over, and it matters considerably.
Summer Surgery: Pros, Cons, and What the Timeline Actually Looks Like
Scheduling rotator cuff surgery at the start of June, the first one to two weeks after the school year ends, is the strategy that works best for most classroom teachers with small-to-medium tears. The rationale is straightforward: the first six weeks of recovery, the highest-risk sling phase, fall entirely within the summer break. Physical therapy begins in weeks two through four and is well underway by August. Many teachers with small tears are cleared for modified classroom duties by late August or early September, allowing a structured re-entry at the start of the new school year.
The important caveat is tear size. Large and massive tears may still require a fall leave period even with optimal summer timing, because the six-month milestone for full duty clearance extends into November or December. A teacher with a massive tear who schedules surgery in June and expects to return unrestricted in September is working from an overly optimistic timeline. A frank conversation with the surgeon about tear size and expected recovery before scheduling is time well spent.
Winter break presents a second viable window, primarily for teachers with small tears and non-dominant arm repairs. The timeline is tighter (typically two weeks of natural break, not twelve), meaning FMLA for the January return to school will likely still be needed, but the start of recovery benefits from uninterrupted rest.
If You Need Surgery During the School Year: What to Plan For
When surgery cannot wait for a break, the planning priority shifts to FMLA paperwork and substitute coverage. Submit FMLA paperwork as early as possible, ideally before surgery, working with HR to designate leave dates. Have the surgeon complete any district-required medical certification forms at the pre-op appointment. Prepare a substitute plan, including lesson materials, classroom routines, and student information, well in advance rather than in the post-op fog of week one.
Signs You Are Ready to Return and Red Flags to Watch For
Readiness for a return to full teaching duties is a clinical question, not a calendar one.
Functional Milestones That Signal Classroom Readiness
Research on return-to-work readiness after rotator cuff repair identifies several functional benchmarks that translate directly to teaching tasks. According to a systematic review published in PeerJ, return-to-work readiness correlates with achievement of full or near-full range of motion, pain-free overhead reach, and shoulder strength at a minimum of 80% of the contralateral (non-operated) side. For teachers, these clinical criteria map onto specific tasks: writing on a whiteboard for ten uninterrupted minutes without pain, lifting a standard ream of paper (approximately five pounds) without discomfort, reaching overhead to a wall shelf, and sustaining keyboard use for thirty minutes without shoulder fatigue. A teacher who cannot perform these tasks without discomfort is not ready for full unrestricted classroom duties, regardless of what week of recovery they are in.
Getting Your Surgical Clearance: What to Ask Your Surgeon
When attending a post-op follow-up and anticipating a return to teaching, come prepared with a specific list of questions. Ask the surgeon to define the exact weight limit for lifting and how long it applies. Ask whether writing on a vertical surface (the whiteboard motion) is cleared or restricted. Ask explicitly about driving clearance, particularly if the dominant arm was repaired. Request a written restrictions note that uses job-specific language rather than generic "light duty" phrasing, because school district HR departments will act on the document language. Ask about re-tear warning signs specifically, including what level of pain or new symptoms should prompt an immediate call to the clinic rather than a wait-and-see approach.
Red flags that suggest too much too soon include a notable increase in shoulder joint-line pain after returning, chronic swelling that does not resolve with rest and ice, a new sensation of catching or clicking inside the joint, or a sudden loss of range of motion that was previously improving. Any of these warrant stepping back from classroom duties and contacting the surgical team promptly.
FAQ
Is rotator cuff surgery minor or major? Rotator cuff repair is classified as a significant orthopedic surgical procedure, not a minor one, because it involves reattaching a tendon to bone under general or regional anesthesia and requires months of structured rehabilitation. It is commonly performed arthroscopically (through small incisions), which reduces soft tissue trauma compared to open surgery, but the biological healing process for the tendon itself is lengthy regardless of technique. Recovery demands genuine time and protection of the repair site.
Can you live alone after rotator cuff surgery? Living alone after rotator cuff surgery is possible, but it requires honest preparation before the procedure. The first two weeks are the most challenging: dressing, bathing, cooking, and driving (particularly with a dominant arm repair) are significantly limited by the sling. Setting up a home environment in advance, including preparing meals, arranging accessible clothing, and moving frequently used items to reachable heights, makes independent recovery considerably more manageable. A doctor can advise on whether specific home circumstances warrant additional support arrangements.
What should you expect twelve weeks after rotator cuff surgery? At twelve weeks, most patients with small-to-medium tears are progressing through the strengthening phase of physical therapy and experiencing meaningful improvement in range of motion. Pain during daily activities should be significantly reduced, though fatigue and achiness with exertion remain common. Many patients report that twelve weeks marks the point where they begin to feel "functional" again, though full strength and endurance typically take another two to three months. For teachers, twelve weeks often aligns with clearance for modified classroom duties if recovery has proceeded on schedule.
How painful is rotator cuff repair surgery? Pain immediately after surgery is managed with a combination of a nerve block (typically lasting twelve to twenty-four hours post-op), prescription pain medication for the first one to two weeks, and over-the-counter anti-inflammatories thereafter. According to Mayo Clinic, the first few days tend to be the most uncomfortable, with pain progressively decreasing over the first two to four weeks. The nerve block wearing off in the first night is a commonly reported challenging moment. Most patients transition off prescription pain medication within two weeks and manage remaining discomfort with non-prescription options.
How do FMLA and summer break interact for teachers? FMLA leave runs concurrently with any leave taken, but here is the key nuance: summer break itself does not count against FMLA entitlement because the employee is not expected to work during that period. A teacher who has surgery in June and returns in September has not consumed any FMLA time if the recovery fell entirely within the summer schedule, assuming they were not on a paid leave designation during that period. A doctor advising on individual circumstances alongside a district HR consultation is the right approach for teachers navigating this intersection, as contract language and district policies vary.
Where can I find more information about navigating my healthcare options during recovery? The Momentary Lab AI Healthcare Navigator can help you understand your diagnosis, explore treatment options, and find relevant questions to bring to your surgical team or HR department.
References
- Haunschild ED, Gilat R, Lavoie-Gagne O, et al. Return to Work After Primary Rotator Cuff Repair: A Systematic Review and Meta-analysis. Am J Sports Med. 2021;49(8):2238-2247. — Systematic review and meta-analysis on return-to-work timing and rates after rotator cuff repair, used for occupational timeline data.
- Mayo Clinic. Rotator Cuff Repair: About This Procedure. — Sourced for post-surgical healing timeline, pain management, and tendon-to-bone biology.
- Cleveland Clinic. Rotator Cuff Repair: Overview. — Sourced for functional recovery timeline of four to six months post-surgery.
- U.S. Department of Labor. Family and Medical Leave Act. — Sourced for FMLA eligibility rules, covered employer definitions, and leave duration.
- ADA National Network. What Is the Americans with Disabilities Act? — Sourced for reasonable accommodation requirements, interactive process obligations, and post-FMLA extended leave framework.
- PeerJ. Systematic Review on Rotator Cuff Repair Return-to-Work Readiness. — Sourced for functional return-to-work milestones including range of motion and strength benchmarks.



