
You've made the decision. The X-rays are filed, the surgery date is circled, and the internet has given you more advice than you can process. But most of what you've read skips the hard parts: the 3 a.m. pain, the emotional crash, the slow-dawning realization that "six weeks and you're back to normal" is nowhere near the truth. This guide covers what surgeons and physical therapists don't always have time to tell you, and what patients say they wish someone had said before they went under.
Whether this is your first question about what I wish I knew before knee replacement surgery or your fifth read-through of the same search results, this is the guide that fills in the gaps.
At a Glance
| Topic | Key Facts |
|---|---|
| Surgery type | Total knee arthroplasty (TKA) or partial knee replacement |
| Average recovery | 12 to 18 months for full healing; 6 weeks for basic mobility |
| Satisfaction rate | Approximately 75 to 80% of patients report good to excellent outcomes |
| Regret rate | Roughly 20 to 25% report ongoing moderate pain at 5 to 8 years |
| Pre-surgery prep | Prehab (strengthening exercises before surgery) measurably improves outcomes |
| Emotional risk | Up to 22 to 33% of patients experience post-surgical depression |
| PT commitment | Daily physical therapy for 8 to 12 weeks post-op minimum |
| Implant lifespan | 15 to 20 years for most modern prosthetics |
The "Why Did I Do This?" Phase: Surviving the First Two Weeks
The first thing nobody tells you clearly enough is this: the first two weeks after knee replacement surgery are genuinely hard, and temporary regret is normal.
You will likely feel worse before you feel better. The knee is swollen, stiff, and painful. The nerve block from surgery wears off, often overnight, and what follows can feel shocking even when you were told to expect it. Patients frequently describe a wave of doubt: "Did I make the right call? Will I ever feel normal again?"
This is sometimes called knee regret, and research suggests it is driven almost entirely by unrealistic expectations set before surgery. A study published through PubMed found that patient satisfaction after total knee arthroplasty is strongly tied to pre-surgical expectations. When patients expect a rapid or complete cure and instead find a slow, painful recovery, dissatisfaction follows even when the surgical outcome is technically excellent.
The acute pain window typically spans days four through seven, after the nerve block has fully resolved and before the strongest anti-inflammatory protocols start making a dent. Sleep is difficult. Getting to the bathroom requires effort and strategy. Dependence on a caregiver feels unfamiliar and uncomfortable.
Acknowledging this phase honestly is not pessimism. It is the single most protective thing a patient can know going in.
"Unrealistic preoperative expectations are associated with worse patient-reported outcomes following total knee arthroplasty." PubMed, 2003

What a Realistic Week-by-Week Recovery Timeline Looks Like
| Milestone | Week 1 to 2 | Week 4 | Week 12 | Week 26 | Week 52 |
|---|---|---|---|---|---|
| Pain level | High; managed with multimodal protocol | Moderate; NSAIDs primary | Mild to moderate with activity | Occasional | Minimal for most |
| Mobility | Walker required; short distances only | Cane possible; stairs with rail | Walking unassisted; light activity | Return to low-impact activities | Near-full function for most |
| PT focus | Knee bends, quad activation, swelling control | Gait training, range of motion goals | Strengthening, balance, functional tasks | Advanced strengthening | Maintenance |
| Activity clearance | Bathroom, short hallway walks | Flat outdoor walking | Driving (left knee: often week 4 to 6; right knee: varies by surgeon) | Swimming, stationary cycling | Light hiking, golf for most patients |
| Sleep quality | Disrupted; position-finding challenging | Improving | Generally stabilized | Normal for most | Normal |
Tissue healing follows biology, not calendars. At six weeks post-surgery, the knee is roughly 10 to 20% healed at the cellular level, according to NIH research on soft tissue repair. Full recovery, including the deep ligament and soft tissue remodeling around the implant, takes 12 to 18 months. Most patients feel functional well before that, but the internal healing process continues long after they stop thinking about it.
Physical Therapy Is a Full-Time Job (and It Hurts)
Physical therapy after knee replacement is not optional, and it is not gentle. That distinction matters.
After surgery, the quadriceps muscle undergoes something called quad shutdown, a neurological inhibition response where the brain temporarily reduces the muscle's ability to contract. Research indicates that patients can lose up to 60 to 80% of quadriceps strength following total knee arthroplasty, according to a review in the NIH National Library of Medicine. Without consistent, deliberate PT work, that strength does not come back on its own.
The stakes of skipping or underperforming in PT are real. The most serious risk is a condition called arthrofibrosis, where excessive scar tissue forms inside the knee joint, permanently limiting range of motion. This can require a second procedure to address. Most surgeons want patients bending the knee to 90 degrees within the first week, which is uncomfortable but achievable with proper technique and pain management.
What PT actually feels like week to week:
During weeks one through two, sessions focus on ankle pumps, heel slides, straight leg raises, and getting the knee to bend far enough to sit in a standard chair. Everything feels stiff and effortful. During weeks three through six, walking pattern and gait correction take center stage alongside progressive strengthening. Weeks seven through twelve shift toward balance work, functional movements like step-ups, and building endurance. The pain during sessions is real but should be described as "discomfort with purpose" rather than sharp warning pain. A good physical therapist will teach patients the difference.
Home compliance matters as much as clinic attendance. Doing assigned exercises twice daily between sessions, even when motivation is low, is the single biggest variable a patient controls in their own recovery.
The Emotional Toll and the Post-Surgery Blues
This is the section most guides skip entirely, and it may be the most important one to read.
Depression after total knee replacement is common. Research published through PMC (PubMed Central) found that 22 to 33% of patients experience clinically significant depressive symptoms following joint replacement surgery. Patients who enter surgery with pre-existing depression or anxiety face a higher risk, and the data shows that depressed patients report worse pain scores and functional outcomes at 12 months compared to those without mood symptoms.
Understanding why this happens makes it less frightening. Several factors converge in the post-operative period: opioid medications can directly alter mood chemistry; the sudden loss of independence creates frustration and grief; the mismatch between expected and actual recovery speed generates anxiety; and the isolation of recovery, especially for people who were previously active, creates a sense of stagnancy.
Patients often describe a specific emotional experience: "I knew I'd be in pain. I didn't know I'd feel so stuck inside my own head."
Signs of Post-Surgery Depression and When to Ask for Help
Clinical depression is not the same as a hard day. If any of the following persist for two or more consecutive weeks, a conversation with a doctor is warranted. Symptoms include persistent low mood or hopelessness, loss of interest in recovery goals, significant changes in appetite or sleep beyond what surgery explains, difficulty concentrating, or thoughts of self-harm.
The connection between narcotic pain medications and mood fluctuation is real and worth tracking. As the opioid component of a pain regimen is reduced or eliminated, many patients notice emotional volatility. This is temporary but can be disorienting if unexpected.
Practical coping strategies that patients report as genuinely helpful include scheduling one social interaction per day even if brief, maintaining a simple daily routine, keeping a progress log to make small gains visible, and being honest with a caregiver or family member about emotional state rather than performing wellness.
If post-surgery depression is suspected, connecting with a physician who can evaluate the full picture is the right step. A doctor can assess whether mood symptoms are medication-related, situational, or require direct treatment.
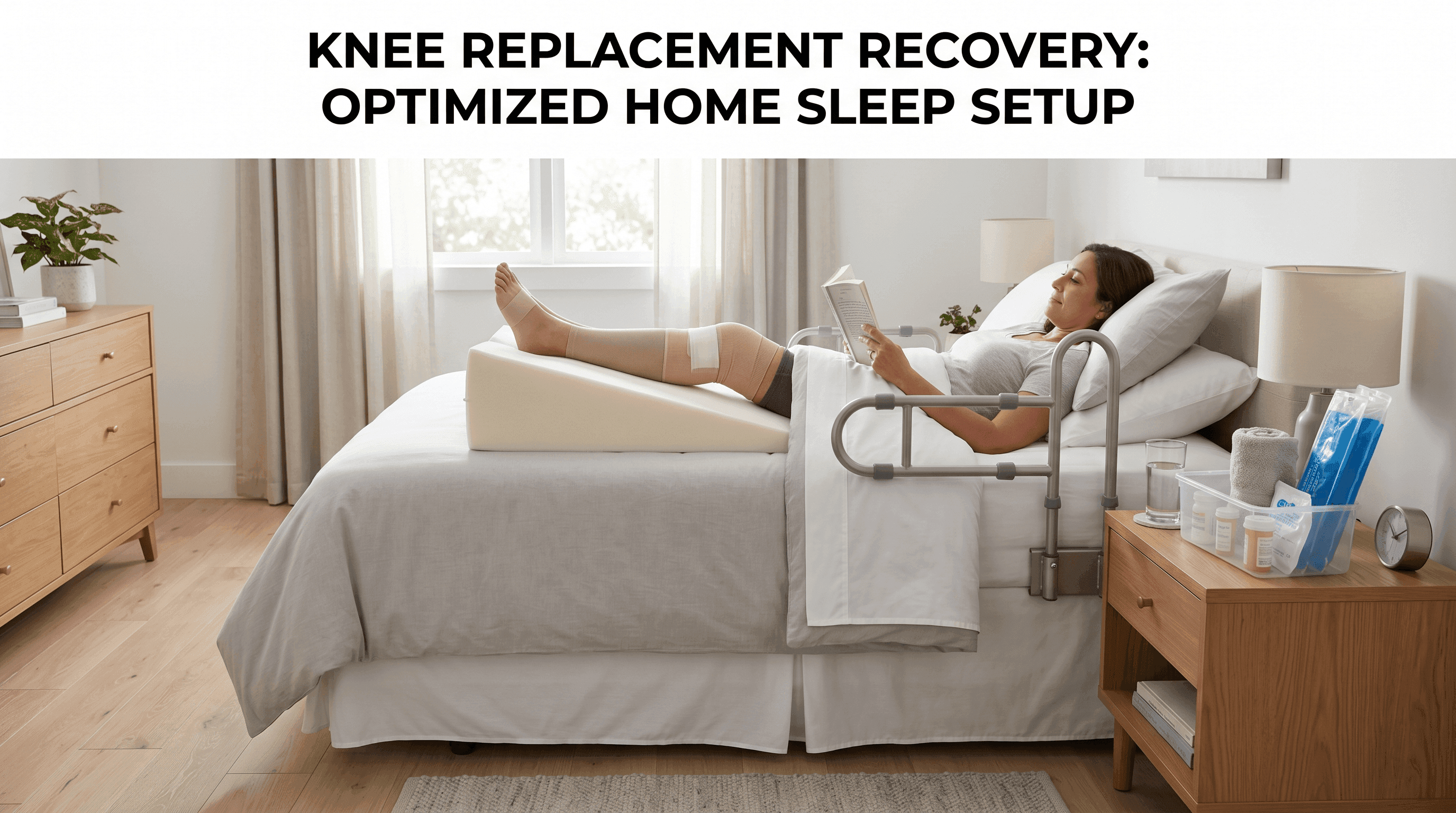
Sleep Will Be Your Biggest Challenge
Sleep deprivation is one of the most consistently underreported struggles of knee replacement recovery, and most pre-surgical conversations give it one sentence at most.
The challenges stack. Finding a comfortable position with a swollen, stiff knee is genuinely difficult. Many patients cannot lie flat comfortably for weeks. The knee often aches more at night when distracting activity stops. Narcotic pain medications disrupt normal sleep architecture even while reducing pain. And the anxiety of recovery, combined with unfamiliar body sensations, keeps the nervous system alert at hours when it should be winding down.
Strategies that help include elevating the operative leg on a firm wedge pillow (not a soft pillow stack, which collapses and provides uneven support), timing pain medication doses to peak coverage during the first sleep cycle, using ice therapy in the hour before bed to reduce inflammation-driven aching, keeping the room cool and dark, and limiting fluid intake in the two hours before sleep to reduce the need to get up.
Most patients find sleep normalizes significantly by weeks four to six as swelling decreases and the need for narcotic medication drops. For patients whose sleep disruption persists beyond six weeks, a conversation with a care team member is appropriate. Poor sleep measurably slows tissue healing and worsens pain perception, making it a medical issue rather than a comfort one.
Pre-Hab: The Pre-Surgery Work That Changes Your Outcome
Prehabilitation, or prehab, refers to targeted strengthening and conditioning performed in the weeks before surgery. It is one of the most evidence-backed investments a knee replacement patient can make, and it remains one of the most underutilized.
The logic is straightforward. Surgery causes immediate muscle weakness. The stronger the surrounding musculature before surgery, the higher the baseline a patient is recovering toward rather than from. Research has consistently shown that patients who complete pre-operative exercise programs experience less post-operative pain, faster return to functional milestones, and better range of motion outcomes compared to those who do not. A meta-analysis cited in the NIH National Library of Medicine confirms that pre-surgical conditioning significantly improves post-operative recovery trajectories.
Prehab also builds neuromuscular familiarity with the movements that PT will demand post-surgery, making the early sessions less foreign and less painful. Patients who have practiced straight leg raises and heel slides before surgery perform them more effectively afterward, when every degree of effort matters.
Upper body and core strength deserve specific mention. Using a walker requires shoulder, arm, and trunk stability. Patients who build this before surgery navigate the walker phase with less strain and fall risk.
Five practical prehab exercises appropriate for most pre-surgical knee patients (always confirm with a surgeon or physical therapist before starting):
Straight leg raises involve lying flat, tightening the quadriceps, and raising the straight leg to about 45 degrees. Quad sets involve pressing the back of the knee into the floor while tightening the quad muscle and holding for five seconds. Short arc quads use a rolled towel under the knee as support while raising the lower leg to full extension. Heel slides, done lying down, involve sliding the heel toward the buttocks and back. Seated knee flexion uses a chair and gravity to gently bend the knee as far as comfortable. Aim for two sets of ten repetitions, twice daily.
Most insurance plans cover prehab physical therapy when prescribed by a surgeon. Asking for that prescription at the pre-surgical appointment costs nothing and may be covered.
The Weird Sensations Are Completely Normal
Two post-surgical experiences catch patients off guard more consistently than any others: skin numbness around the incision, and a clicking or clunking sound from the new joint.
Incision numbness is caused by the surgical disruption of small superficial nerves in the skin around the knee. Most patients notice a patch of numbness, tingling, or altered sensation on the outer side of the knee below the incision. This is not a sign of nerve damage in the dangerous sense. It is a predictable consequence of the surgical approach. For many patients, this numbness persists indefinitely, though the area often shrinks over time as surrounding nerves gradually compensate. A smaller percentage of patients experience complete resolution. Patients should know this before surgery rather than discover it at week three.
Clicking, clunking, or mechanical sounds from the replaced joint are another source of anxiety that rarely needs to be. The prosthetic components are engineered to glide smoothly against a polyethylene bearing surface, and under load or during specific movements like descending stairs, this can produce audible sounds. This is expected, not pathological. A clicking sound that is accompanied by pain, instability, or sudden functional change is worth reporting promptly. An isolated mechanical click without pain or instability is almost universally benign.
Patients also frequently notice increased sensitivity to cold weather in the operative knee. The implant conducts temperature differently than bone does, and many patients describe feeling the metal "feel the cold" in ways their natural knee never did. This is not a complication; it is anatomy.
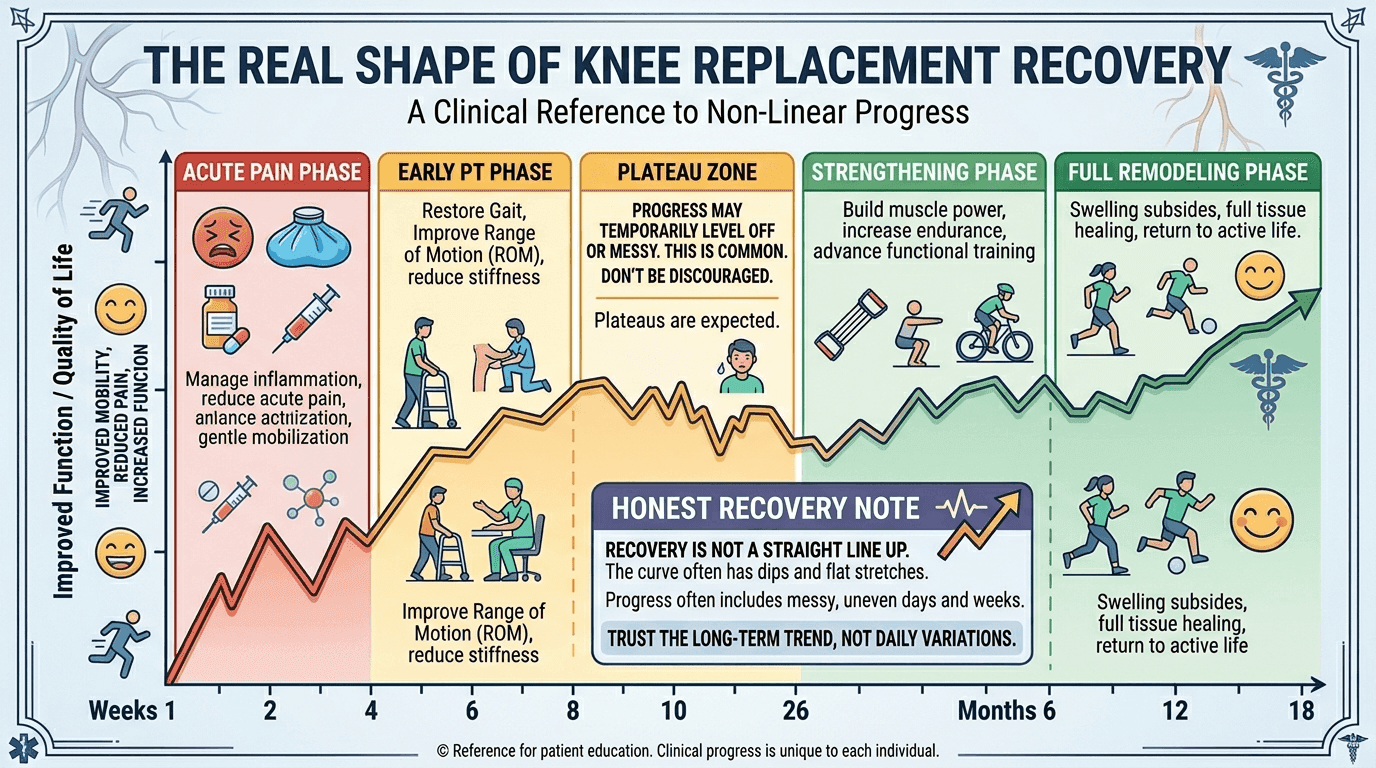
Recovery Is Not a Straight Line
Managing expectations around the recovery arc is the single most practical gift a patient can give themselves before surgery.
The common assumption is linear progress: each week better than the last, trending smoothly toward full function. The reality is different. Most patients experience a notable plateau around weeks six to ten, sometimes called the recovery plateau, where progress feels stalled or even slightly reversed. This is biological, not failure. The inflammatory phase of healing is winding down, and the tissue remodeling phase, which is slower and less perceptible, is taking over.
Flare-ups are also common and normal. A patient who was walking comfortably at week eight may wake up at week ten with a swollen, aching knee after a slightly more active day. This does not mean damage has been done. It means the healing tissue is still communicating its limits. Icing, elevation, a rest day, and returning to activity at a slightly reduced pace is usually all that is required.
The 12-month mark is the more honest benchmark for full recovery, not the six-week mark that gets repeated most frequently. At six weeks, most patients are functional: they can walk without a walker, manage stairs, and begin light activity. But the deep healing, the return of full strength, the resolution of residual aching during weather changes, and the moment the knee stops feeling like a foreign object, these tend to arrive somewhere between months six and twelve.
If the recovery timeline feels overwhelming or confusing at any point, connecting with a qualified orthopedic specialist who knows the full case is the best path forward. Find a doctor on Momentary Lab who can review the surgical plan, physical therapy progress, and any concerns that arise during recovery.
The Ultimate Payoff: Why It Is Ultimately Worth It
After covering the hard parts honestly, this section earns the right to say: for most patients, knee replacement surgery is worth it.
The satisfaction data is meaningful. Between 75 and 80% of total knee replacement patients report good to excellent long-term outcomes, with significant improvements in pain, mobility, and quality of life, according to Harvard Health. Patients return to walking, gardening, traveling, swimming, and participating in daily life in ways that end-stage osteoarthritis had made impossible.
The patients with the best outcomes share common predictors. They entered surgery with realistic expectations. They completed prehab. They adhered to physical therapy even when it was uncomfortable. They had adequate home support in the first two to four weeks. And they understood that recovery is a months-long investment, not a weeks-long inconvenience.
What "the payoff" actually looks like varies by person. For some, it is climbing stairs without gripping the railing. For others, it is sleeping through the night without being woken by joint pain, for the first time in years. For many, it is simply walking across a parking lot without planning the route around benches.
One patient's account, shared in a clinical review context: "By month nine, I forgot which knee it was. That was the moment I knew it worked."
The research and the patient experience align on one consistent truth. Informed, prepared patients have measurably better outcomes than those who enter surgery without fully understanding what is ahead. Reading this guide is itself a form of preparation.
The Most Important Thing to Do Right Now
Preparation, physical, logistical, and emotional, is the strongest predictor of a good knee replacement outcome that a patient can influence.
Start prehab now if surgery is weeks away. Set up the home before the surgery date, not after. Have an honest conversation with a caregiver about what the first two weeks will actually require. And give yourself permission to have hard days without interpreting them as failure.
The discomfort of recovery is finite. The improvement, for the majority of patients who prepare well, is lasting.
For trusted health information and help navigating care options throughout recovery, the Momentary Lab AI Healthcare Navigator can point toward resources, explain medical terminology, and help formulate questions before the next appointment.
FAQ
What are the five mistakes people make after knee replacement?
The most common mistakes are skipping or underperforming in physical therapy, expecting a linear recovery without plateaus or flare-ups, not preparing the home before surgery (leading to fall risk and unnecessary pain), stopping pain medication too abruptly before consulting the care team, and ignoring emotional symptoms like post-surgical depression. Each of these mistakes is avoidable with preparation and honest expectation-setting before the procedure.
What is the regret rate for knee replacement surgery?
Roughly 20 to 25% of patients report ongoing moderate pain or dissatisfaction at five to eight years post-surgery. However, research consistently shows that a significant portion of this dissatisfaction is linked to unrealistic pre-surgical expectations rather than surgical failure. Patients who entered surgery with clear, accurate expectations about recovery time and functional outcomes report substantially higher satisfaction rates.
What can you never do after a knee replacement?
Most surgeons advise patients to avoid high-impact activities permanently, including running, jumping, and contact sports. Activities that place extreme torque on the joint, such as skiing moguls or squash, are also typically discouraged. Activities that are generally well-tolerated long-term include walking, swimming, cycling, golf, and light hiking. The specific restrictions depend on the implant type and individual case, so a direct conversation with the operating surgeon is the most reliable source of guidance.
What don't they tell you about knee replacements?
Several things tend to get underemphasized before surgery. The skin numbness around the incision that persists for months or permanently in many patients surprises nearly everyone. The mechanical clicking sound of the prosthetic components is common and normal but rarely mentioned. Post-surgical depression affects up to a third of patients and is not routinely screened for. Sleep disruption is severe in the first two to four weeks and requires specific strategies. And full recovery takes 12 to 18 months, not the six weeks that many patients take away from pre-surgical conversations.
How painful is physical therapy after knee replacement?
Physical therapy after knee replacement is uncomfortable, particularly in the first six weeks. The goal of early PT is to achieve specific range of motion benchmarks, including 90-degree knee flexion in the first week, and this requires pushing past resistance and stiffness. Patients consistently describe it as "the kind of pain that means progress." Sharp, electrical, or shooting pain is different and should be communicated to the therapist immediately. The discomfort of PT is managed through timing exercises with peak medication effect and using ice afterward.
How do I know if I am a candidate for outpatient knee replacement?
Outpatient (same-day discharge) knee replacement is increasingly common for appropriately selected patients. General candidate factors include a BMI under 40, no significant uncontrolled comorbidities such as severe cardiac disease or poorly controlled diabetes, reliable home support for the first 24 to 48 hours, a home environment that is reasonably accessible, and a surgeon who performs high enough annual volume to support safe same-day protocols. The American Association of Hip and Knee Surgeons has found equivalent outcomes between outpatient and inpatient settings when patients are properly screened. This is a conversation to have directly with the surgical team well before the procedure date.
References
- PubMed, Bourne et al., 2003 — Cited for data on patient expectations and satisfaction outcomes after total knee arthroplasty.
- PMC, PubMed Central, 2018 — Cited for prevalence of post-surgical depression (22 to 33%) and its effect on WOMAC scores and functional outcomes at 12 months.
- NIH National Library of Medicine, StatPearls, Total Knee Arthroplasty — Cited for soft tissue healing timelines and pre-surgical conditioning outcomes.
- NIH National Library of Medicine, StatPearls, Physical Therapy Knee — Cited for quadriceps strength loss post-surgery (up to 60 to 80%) and neuromuscular rehabilitation evidence.
- Harvard Health, "Time for a New Knee? Ask These Questions First" — Cited for long-term satisfaction rates (75 to 80%) and questions to ask before surgery.



