
Recovering from rotator cuff surgery is a study in patience, and the most common question patients bring to their six-month follow-up is a simple one: "When can I finally lift something heavy again?" If you have a job that demands it, a sport you want to return to, or just a box in the garage that needs moving, this article gives you the concrete answer your surgeon would give, along with all the nuance that goes with it.
At a Glance
| Topic | Key Facts |
|---|---|
| Target milestone | 50 lbs typically cleared at months 5 to 6 (waist level) |
| Sling phase | Weeks 0 to 6: zero lifting |
| Light lifting begins | Around week 6 to 8 (1 to 2 lbs only) |
| 10 lbs to waist | Around month 3 |
| 25 lbs to waist | Around month 4.5 |
| 50 lbs clearance | Month 6 with surgeon approval |
| Overhead 50 lbs | Typically months 9 to 12 or later |
| Re-tear risk | 15 to 21% overall within the first year |
| Full recovery timeline | 9 to 12 months for complete healing |
The Short Answer — Why Heavy Lifting Takes 6 to 9 Months
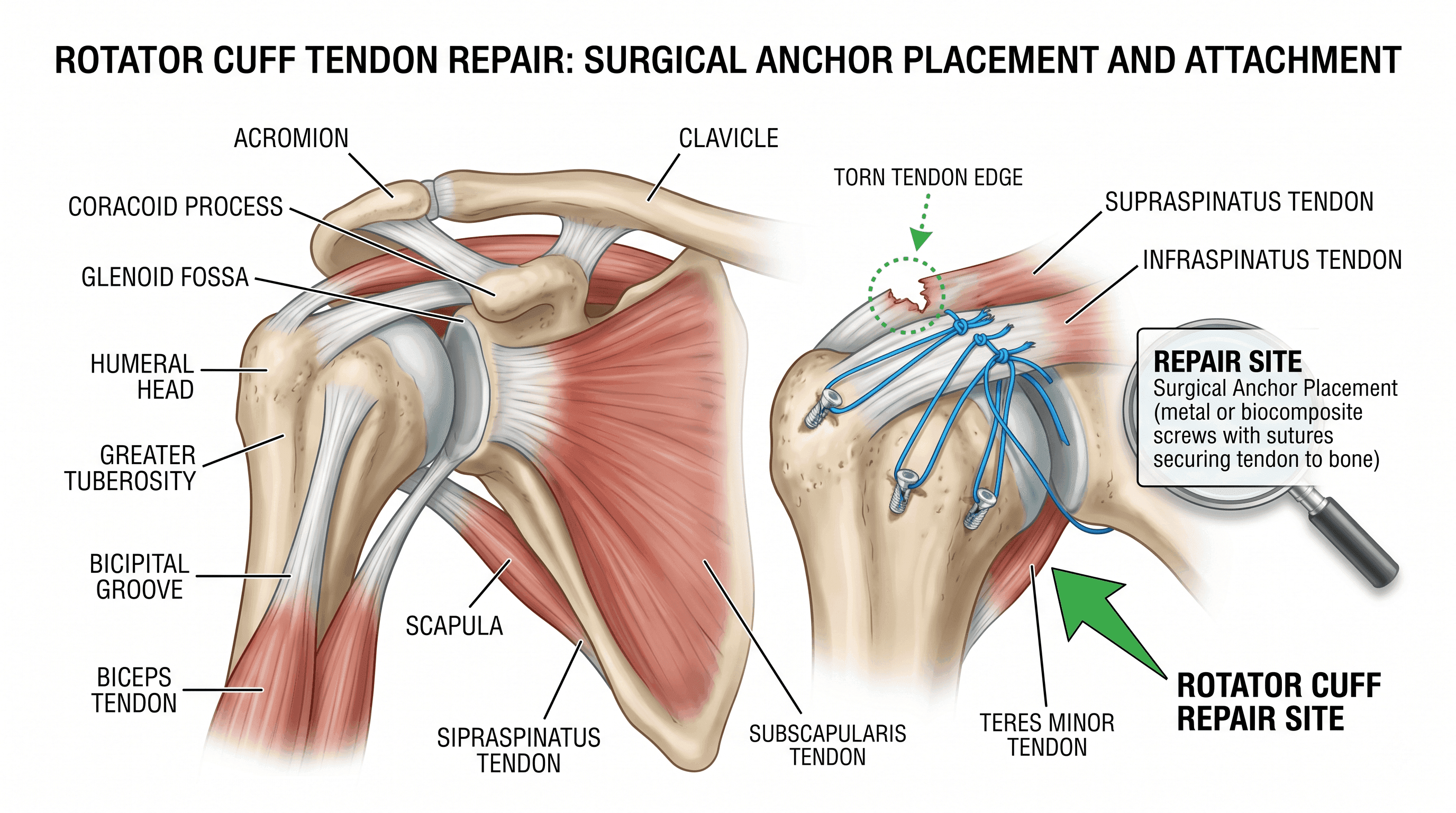
Most patients receive clearance to lift 50 pounds at waist level somewhere between months 5 and 6, but only after a surgeon confirms the repair has healed adequately. That timeline is not arbitrary. Rotator cuff surgery anchors a torn tendon back to bone using small surgical suture anchors, and the tendon has to regrow its biological attachment at the cellular level before it can handle significant load.
According to the Mayo Clinic, rotator cuff repairs require a protected recovery period of several months because the repaired tendon is vulnerable to re-tear until full tissue integration occurs. Fifty pounds is a meaningful mechanical load on any shoulder, and at the waist level it still recruits the rotator cuff significantly. Overhead, 50 pounds is a different challenge entirely, and most surgeons push that clearance to nine months or beyond.
The most important thing to understand early: feeling strong does not mean the repair is ready. Muscle soreness fades, pain subsides, and range of motion returns, sometimes weeks before the actual tendon-to-bone junction is mature enough to handle load. A patient who feels "good enough" at three months and tests a heavy lift is gambling on a repair that is still completing its cellular integration.
The Biology of Healing — Why You Cannot Rush the Timeline
Tendon-to-bone healing after rotator cuff repair follows three distinct biological phases. Research published in PMC via NIH describes these as the inflammatory phase (approximately seven days), the proliferative phase (two to three weeks), and the maturation or remodeling phase, which spans roughly 12 to 26 weeks after surgery. Each phase must progress before loading the repair makes biological sense.
The maturation phase is what most patients do not hear about. By six weeks, the inflammatory and early repair activity has largely progressed, but the structural anchoring of tendon to bone is still incomplete. Research on primate models, published in NIH-indexed literature and summarized in PMC, found that the specialized connective fibers that bind a healing tendon to bone did not appear in meaningful numbers before week 12. By week 15, the bone-tendon junction approached maturity. The same body of work found that repair strength in animal models was likely below 30% of normal at six weeks and no more than 50% of normal at 12 weeks.
This is the central reason lifting restrictions exist in stages rather than as a single cutoff date. At six weeks, the repair looks healed from the outside. Internally, the structural scaffolding is still forming.
What this means practically: your muscles may recover faster than your repair site. Strength in the surrounding deltoid or biceps can mask tendon vulnerability. The timeline is set not by how your arm feels, but by where the biology is in its healing sequence.
The Weight Progression Timeline (Phase by Phase)
The following timeline reflects a standard arthroscopic rotator cuff repair protocol synthesized from clinical protocols including those published by TCOMN/Dr. Kelly and rehabilitation guidelines from Mass General Hospital. Individual protocols vary by surgeon, tear size, and repair type. Always defer to your own surgical team.
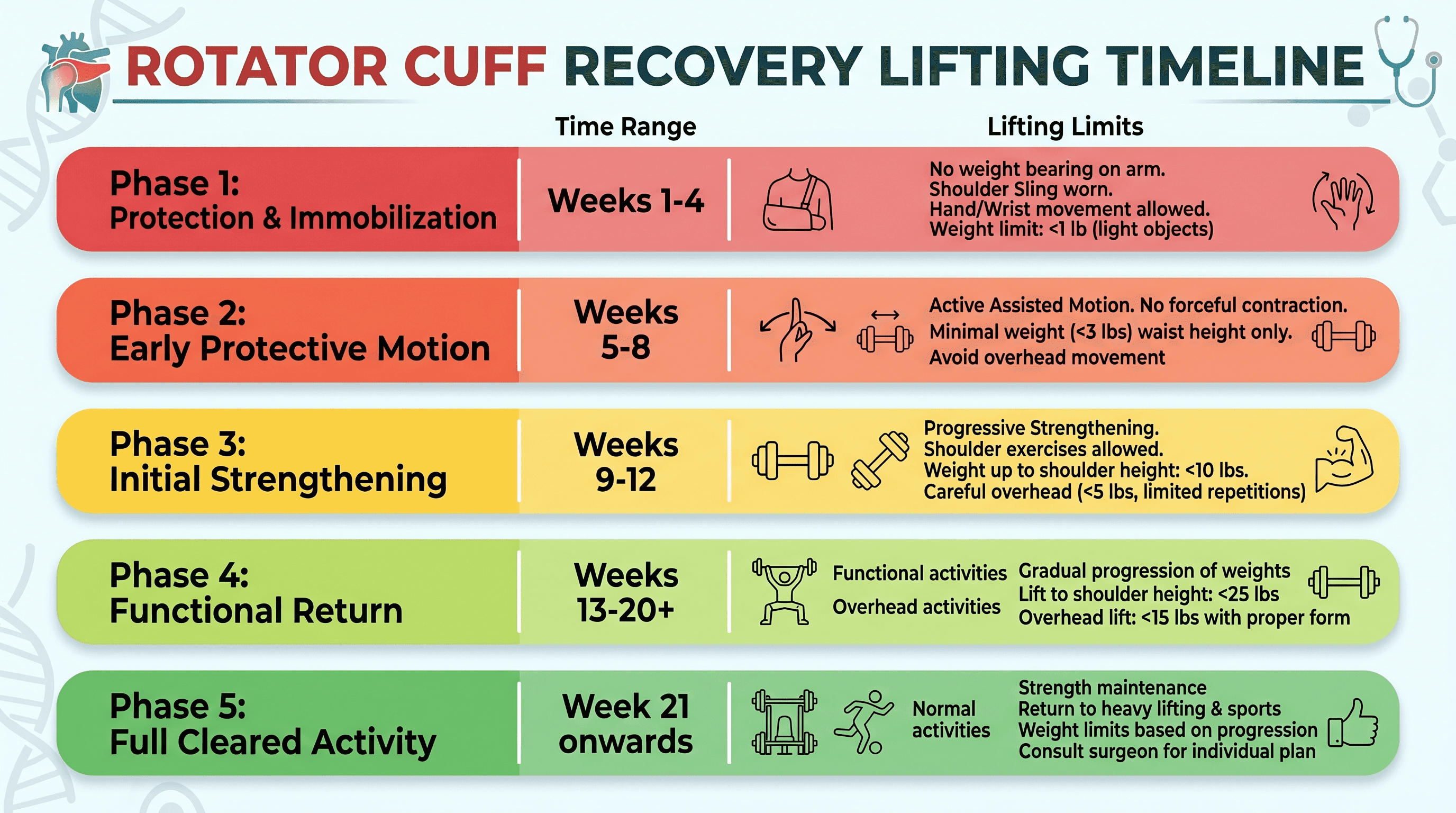
| Phase | Weeks | Waist-Level Limit | Shoulder-Level Limit | Overhead Limit |
|---|---|---|---|---|
| Phase 1 (Sling) | 0 to 6 | 0 lbs | 0 lbs | 0 lbs |
| Phase 2 (Early Motion) | 6 to 12 | 1 to 2 lbs | None | None |
| Phase 3 (Strengthening) | 12 to 18 | 10 lbs | 5 lbs | 2 lbs occasionally |
| Phase 4 (Progressive Load) | 18 to 24 | 25 lbs | 10 lbs | 5 lbs |
| Phase 5 (Full Activity) | Month 6+ | Surgeon-cleared (up to 50+ lbs) | Surgeon-cleared | Surgeon-cleared |
Phase 1 — Sling Phase (Weeks 0 to 6)
The arm rests in a sling at all times, including during sleep. Zero lifting is the rule, no exceptions. The tendon is at its most vulnerable during this window. Physical therapy during this phase is passive only, meaning a therapist moves your arm while your muscles stay relaxed. The goal is preventing scar tissue formation (adhesive capsulitis) without placing any stress on the repair.
Phase 2 — Early Active Motion (Weeks 6 to 12)
The sling comes off around week six, and active range of motion begins under PT guidance. Lifting is restricted to roughly one to two pounds, the weight of a coffee mug. Isometric exercises are introduced with sub-maximal effort only. The MGH protocol explicitly notes that maximal activation at this stage can overload the repair.
Phase 3 — Progressive Strengthening (Weeks 12 to 18)
Resistance training becomes more structured. Most patients can lift up to 10 pounds to waist level, five pounds to shoulder height, and occasionally two pounds overhead. This is the phase where compensatory movement patterns (shrugging, leaning) need to be corrected by a physical therapist before loads increase further.
Phase 4 — Progressive Loading (Weeks 18 to 24)
Lifting limits step up to 25 pounds at waist level, 10 pounds to the shoulder, and five pounds occasionally overhead. Patients with physically demanding jobs often begin work-conditioning programs during this window.
Phase 5 — Surgeon-Cleared Full Activity (Month 6+)
At the six-month visit, surgeons typically release patients from all formal restrictions, provided the repair has progressed appropriately. This is when 50-pound lifting at waist level becomes a realistic target for most patients.
Waist-Level vs. Overhead Lifting — Why the Difference Matters
The position of your arm during a lift changes which muscles and repair structures bear the load, and by how much. This distinction is clinically meaningful and explains why a patient cleared to carry a grocery bag at waist height still cannot press overhead without restriction.
When you lift from the floor or waist level, the load is primarily distributed through your forearm, elbow, and the large muscles of the back and biceps. The rotator cuff acts as a stabilizer in this position but does not bear the full lifting force. This is why waist-level lifting restrictions clear first and do so earlier.
Overhead lifting is an entirely different biomechanical story. Raising the arm above shoulder height requires the rotator cuff muscles, particularly the supraspinatus, to work at their highest mechanical disadvantage. The repaired tendon is under greater tension and shear force. Pressing or carrying 50 pounds overhead before full tissue maturity is asking a repair site that may be at 50 to 60% structural capacity to handle a near-maximal load.
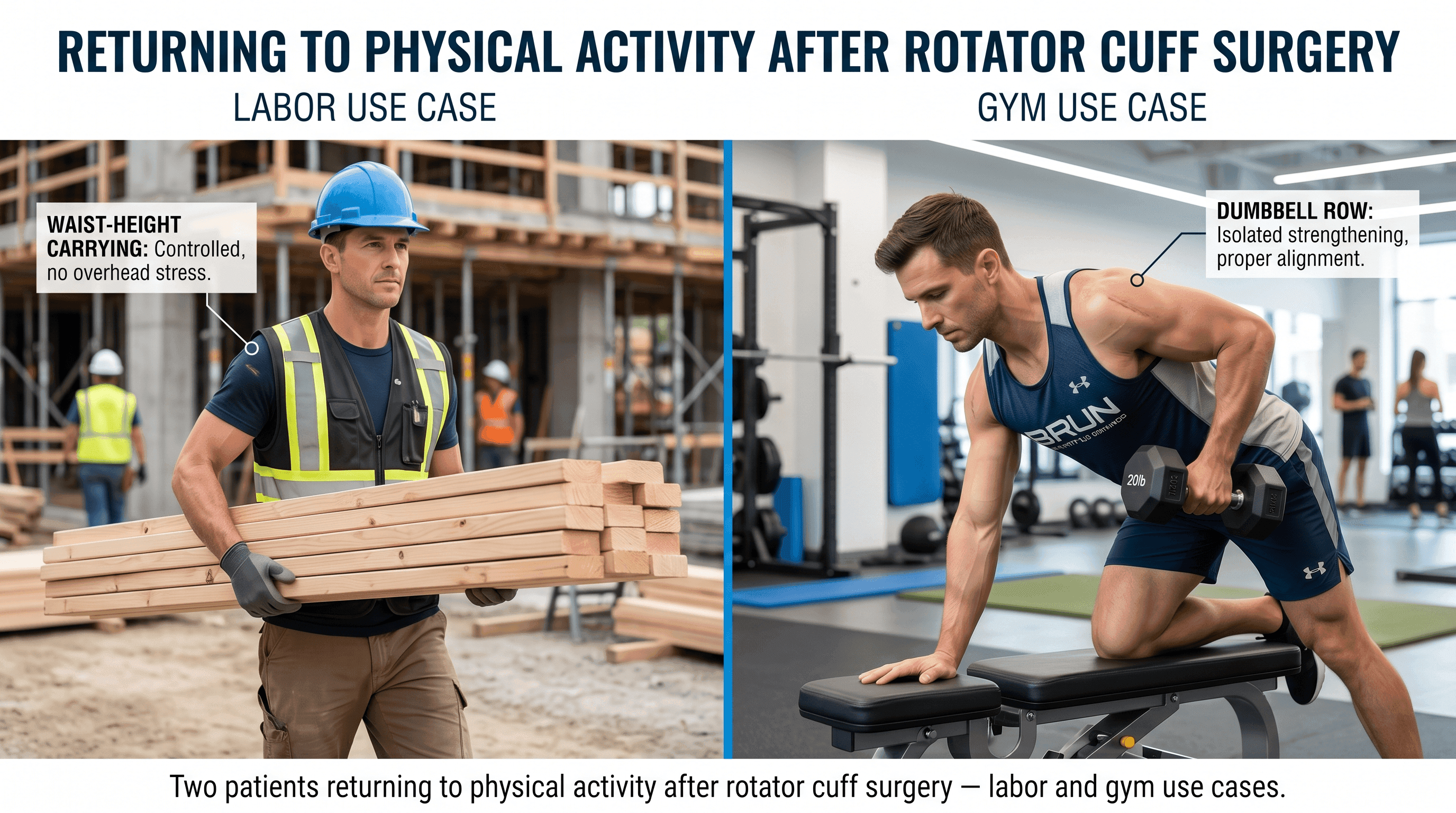
The practical takeaway: if your job involves carrying 50 pounds at waist level (think warehouse floor work, moving equipment from a cart), you may reach clearance closer to month 5 or 6. If your job involves lifting 50 pounds overhead repeatedly (construction overhead work, certain nursing transfers), expect a 9 to 12-month timeline and a more gradual return pathway.
The Danger of Testing It Too Early — Understanding Re-Tear Risks
Re-tear after rotator cuff repair is a real and documented risk, not a theoretical one. A large database review of 98,844 patients published in ScienceDirect found an overall re-tear rate of 16.3% within one year of surgery. A separate NIH-indexed review put the re-injury incidence between 15% and 21% depending on tear severity and patient factors. For massive tears or older patients, that number climbs higher.
Re-tears from premature loading are mechanically straightforward. The suture anchors hold the tendon in position while new biological attachment forms. If a significant load is applied before those cellular connections mature, the repair can fail at the anchor-to-tendon interface. In many cases this requires revision surgery, which carries a longer and more uncertain recovery than the original procedure.
Warning signs that something may have gone wrong after a lift include a sudden sharp pain in the shoulder, significant swelling or warmth that was not present before, a noticeable pop or giving-way sensation, or a rapid loss of strength that follows the lift. Any of these deserve a prompt call to your surgeon.
The comorbidities most strongly associated with elevated re-tear risk are smoking, hypertension, and elevated lipid levels. According to that same large-scale database study, patients aged 81 to 90 had the highest relative re-tear risk at 19.6%. Age is among the most consistent predictors of poorer structural healing after rotator cuff repair, and this informs why older patients are often held to more conservative timelines.
Returning to Heavy Labor and Construction Jobs
For patients whose livelihood depends on 50-pound or heavier lifting, returning to work is not just a medical milestone but a financial one. The honest answer for most physically demanding roles is that safe, unrestricted return to heavy labor typically falls between months 6 and 9, and in some cases longer.
Physical Jobs: Construction, Nursing, Warehouse Work
Patients returning to construction, warehouse work, or physically demanding healthcare roles (patient transfers, repositioning) are generally cleared for full duty between months 6 and 9. Surgeon clearance alone may not be sufficient. Most occupational medicine programs and workers' compensation systems require formal documentation that a patient can safely perform job-specific tasks before reinstating full duty status.
Work conditioning programs, offered by specialized physical therapy and occupational therapy clinics, are designed specifically for this transition. These programs simulate the physical demands of a given job and progressively build the shoulder's capacity to handle those loads over several weeks. If you are returning to a labor role, speak with your PT about a formal work conditioning referral starting around month 4 or 5.
Gym and Recreational Weightlifting
For gym-goers and recreational lifters, a progressive return to barbell and dumbbell training typically begins around month 3 with very light loads, using the weight restrictions outlined in the phase table above. The 50-pound benchmark for exercises like dumbbell rows or loaded carries becomes achievable around month 5 to 6 for most patients.
Movements that place the shoulder under load at the end range, such as behind-the-neck press, wide-grip bench press, and deep cable flies, carry higher re-tear risk and should be reintroduced cautiously even after general clearance. A physical therapist with sports rehab experience can help redesign a training program that protects the repair while maintaining conditioning.
Overhead Sports and Throwing Athletes
Baseball, softball, volleyball, and similar overhead sports require the most conservative timelines. Throwing athletes and overhead sport participants should generally expect a 9 to 12-month return-to-sport timeline, with sport-specific throwing or hitting programs beginning no earlier than month 6 and only after strength symmetry testing confirms the repaired shoulder is within roughly 90% of the unaffected side.
Passing the Functional Capacity Evaluation (FCE) for Heavy-Duty Work
For patients in jobs covered by workers' compensation or disability claims, or those returning to physically demanding roles that require documented medical clearance, a Functional Capacity Evaluation (FCE) is often the formal gateway back to full duty.
An FCE is a standardized assessment conducted by a licensed physical or occupational therapist that measures a patient's actual physical capacity against the specific demands of their job. Cleveland Clinic's Return to Work program describes the FCE as a process that assesses functional abilities including material handling capacities, consistency of effort, and reliability, and that establishes formal return-to-work status.
For a rotator cuff patient, the FCE typically tests: lifting and carrying tasks at floor, waist, and shoulder height; pushing and pulling force; grip and pinch strength using a dynamometer; and job-specific simulations relevant to the patient's actual work tasks. The evaluation usually runs two to four hours in a single session.
Passing an FCE does not simply mean "feeling ready." It means demonstrating, under objective measurement, that the repaired shoulder can safely meet the physical demands of a specific role. Patients who attempt an FCE too early, before completing the full rehab progression, often do not pass and must wait for a repeat evaluation.
If you need an FCE as part of your return-to-work process, ask your surgeon for a referral to a certified provider, typically a work rehabilitation or occupational health clinic. Scheduling it around month 5 to 6, after progressing through the formal lifting phases, gives most patients the best chance of passing the first time.
If you are unsure whether your shoulder is ready for this evaluation or what specialists in your area offer FCE services, find a doctor near you who can coordinate your post-surgical care and provide the appropriate referrals.
Long-Term Gym Protocols — Returning to Weightlifting
For athletes and regular gym-goers, the question after 50-pound clearance is what comes next, and how to train smart without jeopardizing a repair that took months to protect.
After surgeon clearance at or around month 6, the guiding principles for returning to structured weightlifting are progressive overload with controlled mechanics, avoidance of end-range loading until month 9 to 12, and ongoing attention to compensatory patterns.
Exercises that are generally reintroduced earlier (months 6 to 9):
Neutral-grip rows, lat pulldowns with a shoulder-width grip, light to moderate dumbbell pressing at or below shoulder height, loaded carries at waist level, and machine-based pulling movements are among the lower-risk options during this window. These keep the shoulder in its stable mid-range and avoid the positions of highest mechanical disadvantage.
Exercises to reintroduce cautiously (months 9 to 12 or later):
Overhead pressing movements, behind-the-neck work, wide-grip barbell bench press, and any movement requiring the shoulder to bear load at the end of its range are introduced later and with clinical guidance. These movements are not permanently off the table for most patients; they require a longer runway.
What the evidence supports for preserving muscle during recovery:
Blood flow restriction (BFR) training has gained traction in post-surgical rehabilitation as a way to preserve muscle mass with very low external loads during the earlier phases. A physical therapist trained in BFR can introduce this starting around weeks 6 to 12, allowing metabolic stimulus without the mechanical load that could compromise the repair.
Protein intake and sleep are also worth deliberate attention during recovery. Tendon remodeling is a metabolic process, and adequate dietary protein supports the synthesis of new connective tissue. If you are a smoker, cessation is not just a general health recommendation here: the evidence clearly links smoking to elevated re-tear risk and poorer structural healing outcomes.
Frequently Asked Questions
How long after rotator cuff surgery can I lift 20 pounds?
Most protocols allow up to 10 pounds at waist level at the three-month mark, and progression to 25 pounds around month 4.5. Reaching 20 pounds consistently and comfortably typically falls between months 3 and 4.5, depending on how the strengthening phase progresses. Your surgeon or physical therapist will confirm based on your specific repair.
How long does it take for tendons to reattach to bone after rotator cuff surgery?
According to NIH-published research, the maturation phase of tendon-to-bone healing spans roughly 12 to 26 weeks after surgery. Histological studies show the specialized fibers that bind tendon to bone do not appear in significant numbers before week 12, and approach structural maturity closer to week 15. Full biological consolidation continues for up to 6 months.
Can you do bicep curls after rotator cuff surgery?
Light bicep curls typically reappear in rehab programs around weeks 12 to 18 with very limited weight. If a bicep tenodesis was performed alongside the rotator cuff repair, bicep-loading restrictions may be stricter and more prolonged. Always confirm with your surgical team before starting any bicep loading, as the tenodesis site has its own healing timeline.
What movements should I permanently avoid after rotator cuff surgery?
Most patients with successful repairs return to full activity over time and do not face permanent restrictions. That said, high-impact overhead movements, repeated heavy overhead pressing, and throwing sports should be reintroduced very gradually with PT guidance. Some patients with massive or complex repairs are counseled to avoid repetitive overhead loading long-term to protect the repaired tissue. A doctor can advise on individual cases based on the extent of the original tear and the surgical repair achieved.
Is 50 lbs a permanent lifting limit after shoulder surgery?
No. For most patients, 50 pounds at six months is not a ceiling, it is a milestone. After surgeon clearance and successful FCE (where required), many patients return to lifting well beyond 50 pounds for work, sport, and daily life. Overhead loading beyond 50 pounds may take longer, particularly for massive tears or older patients.
When can I carry groceries after rotator cuff surgery?
Carrying standard grocery bags, which typically weigh between 5 and 15 pounds, becomes feasible around months 2 to 3 for most patients. A single bag at waist level is within the 10-pound limit set at the three-month mark. Avoid carrying bags with your arm extended away from your body, which places greater load on the repair. A rolling cart or carrying close to your body at this stage is a practical workaround.
For personalized guidance on your recovery timeline, exploring your rehabilitation options, or understanding what your surgical report means for your lifting milestones, the Momentary Lab AI Healthcare Navigator can help you find relevant information and connect with the right care resources.
References
- NIH PMC — Rehabilitation after Rotator Cuff Repair — Cited for three-phase healing biology (inflammatory, proliferative, maturation phases) and immobilization protocol guidance.
- NIH PMC — Rotator Cuff Repair Rehabilitation Considerations — Cited for Sharpey's fiber formation timeline, structural maturity at week 15, and repair strength data at 6 and 12 weeks.
- NIH PMC — Rotator Cuff Repair Post-Op Rehabilitation Concepts — Cited for the three-stage healing process and early passive motion research.
- TCOMN / Dr. Kelly Rotator Cuff Repair Post-Op Handout — Cited for phase-by-phase lifting restriction milestones (waist, shoulder, overhead limits by month).
- Mass General Hospital Rehab Protocol — Large to Massive Tear — Cited for isometric strengthening timing and sub-maximal activation guidance.
- ScienceDirect — TriNetX Database Review of 98,844 Patients — Cited for 16.3% overall re-tear rate, smoking and hypertension as risk factors, and age-related re-tear statistics.
- NIH PMC — Risk Factors, Incidence, and Management of Rotator Cuff Re-Injury — Cited for 15% to 21% re-injury incidence range and age as the strongest predictor of re-tear.
- Mayo Clinic — Rotator Cuff Injury — Cited for protected recovery period rationale and passive motion guidance.
- Cleveland Clinic — Return to Work Services — Cited for FCE definition, functional abilities assessment, and return-to-work status determination.



