
Recovery from rotator cuff surgery raises one question above all others: when does physical therapy begin? The honest answer is that it depends, and no single timeline fits every patient. Your surgeon's protocol, the size of the tear, and the complexity of the repair all shape the answer. But most patients begin some form of PT between 3 days and 6 weeks after surgery — and understanding why that range exists will help you make sense of your own plan.
At a Glance
| Topic | Key Facts |
|---|---|
| Typical PT start window | 3 days to 6 weeks post-surgery |
| First PT phase | Passive range of motion only (therapist moves the arm) |
| Early protocol candidates | Small tears under 3 cm, strong tendon tissue |
| Delayed protocol candidates | Massive tears, poor tissue quality, subscapularis repairs |
| Primary early goal | Preventing frozen shoulder (adhesive capsulitis) |
| Risk of starting too soon | Retear of the surgically repaired tendon |
| Risk of starting too late | Permanent stiffness, prolonged recovery |
The Short Answer: It Can Range from 3 Days to 6 Weeks
The range is not a hedge. It reflects a genuine clinical reality: rotator cuff surgery is not one procedure, and every repaired shoulder heals on its own terms.
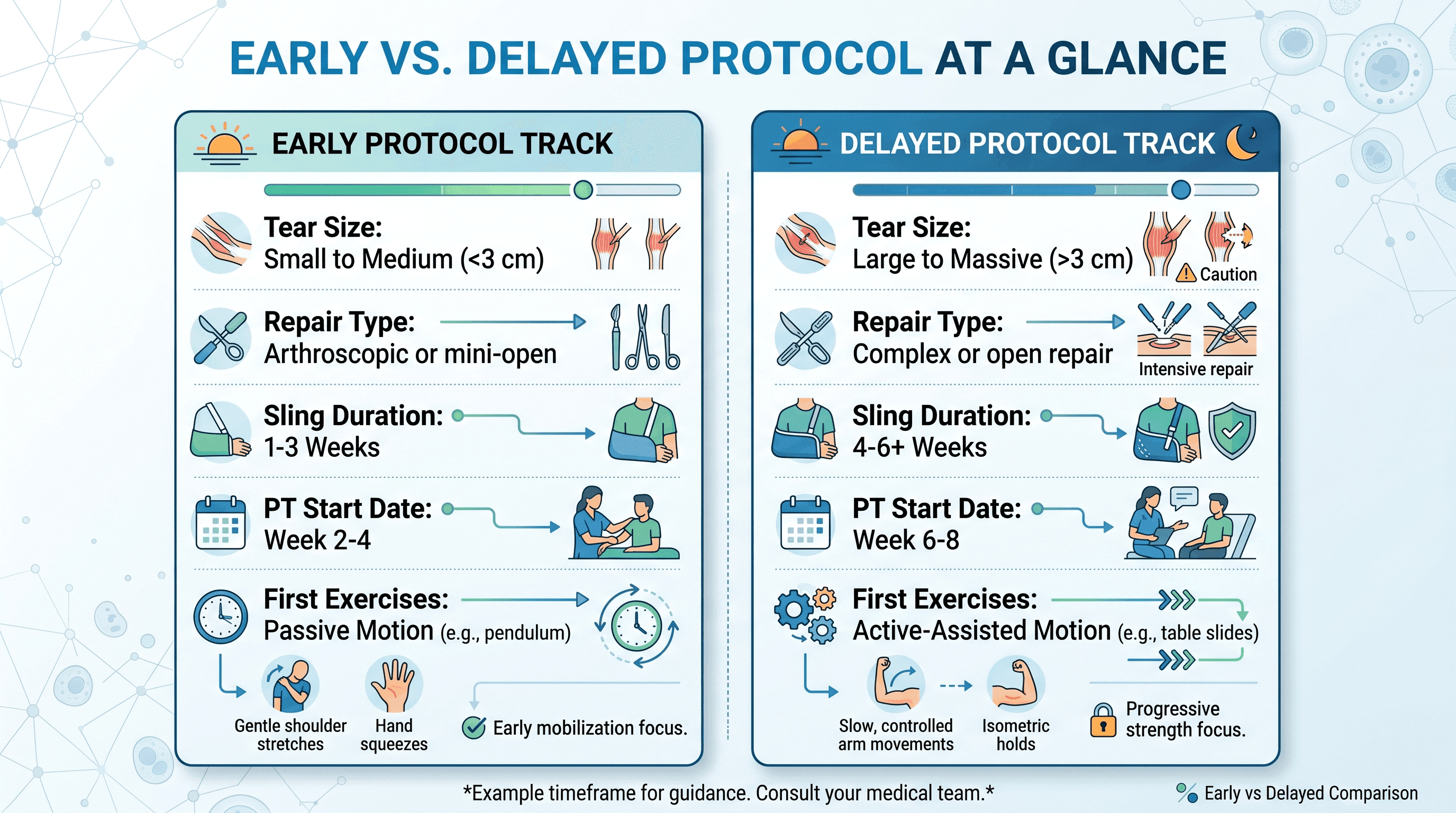
For patients with smaller, straightforward tears, research supports early mobilization. A 2023 meta-analysis published in BMC Musculoskeletal Disorders found that early mobilization was safer for tears under 3 cm, with retear risk remaining acceptably low when passive motion began within the first two weeks. For larger tears, however, the same research noted a meaningfully higher retear risk with early movement. That distinction alone explains most of the variation patients encounter.
Three variables drive the start date: the size of the tear before surgery, the quality of the tendon tissue the surgeon worked with, and the specific repair technique used. A surgeon repairing a small, clean tear in healthy tissue will almost always clear PT sooner than one who reconstructed a massive tear with a complex anchor pattern. Neither approach is wrong. They reflect different tissue realities.
The Surgical Tug-of-War: Stiffness vs. Healing
Every post-operative rotator cuff shoulder sits at the center of a biological tug-of-war. On one side, the repaired tendon needs stillness to lay down collagen fibers and attach firmly to bone. On the other, a motionless shoulder begins forming scar tissue within days of surgery, and that scar tissue can calcify into the debilitating stiffness known as adhesive capsulitis, or frozen shoulder.
Your surgeon and physical therapist are managing both sides of this equation simultaneously. Moving the shoulder too early can pull anchors loose before the tendon-to-bone attachment has time to mature. Waiting too long allows scar tissue to organize in ways that may require a second procedure to correct. The PT start date is the inflection point where those two risks are balanced against each other for your specific shoulder.
According to the University of Iowa MOON Rotator Cuff Repair Immediate Therapy Protocol, some patients are cleared for passive motion exercises beginning the day after surgery, while others remain in a strict sling with no PT for four to six weeks. The deciding factor in most protocols is not the patient's pain tolerance or motivation; it is the integrity of the repair as the surgeon assessed it in the operating room.
The Crucial Difference: Passive vs. Active Motion
One of the most important things to understand before your first PT appointment is that early physical therapy after rotator cuff surgery is not what most people picture. There are no resistance bands on day three. There are no overhead presses at week two.
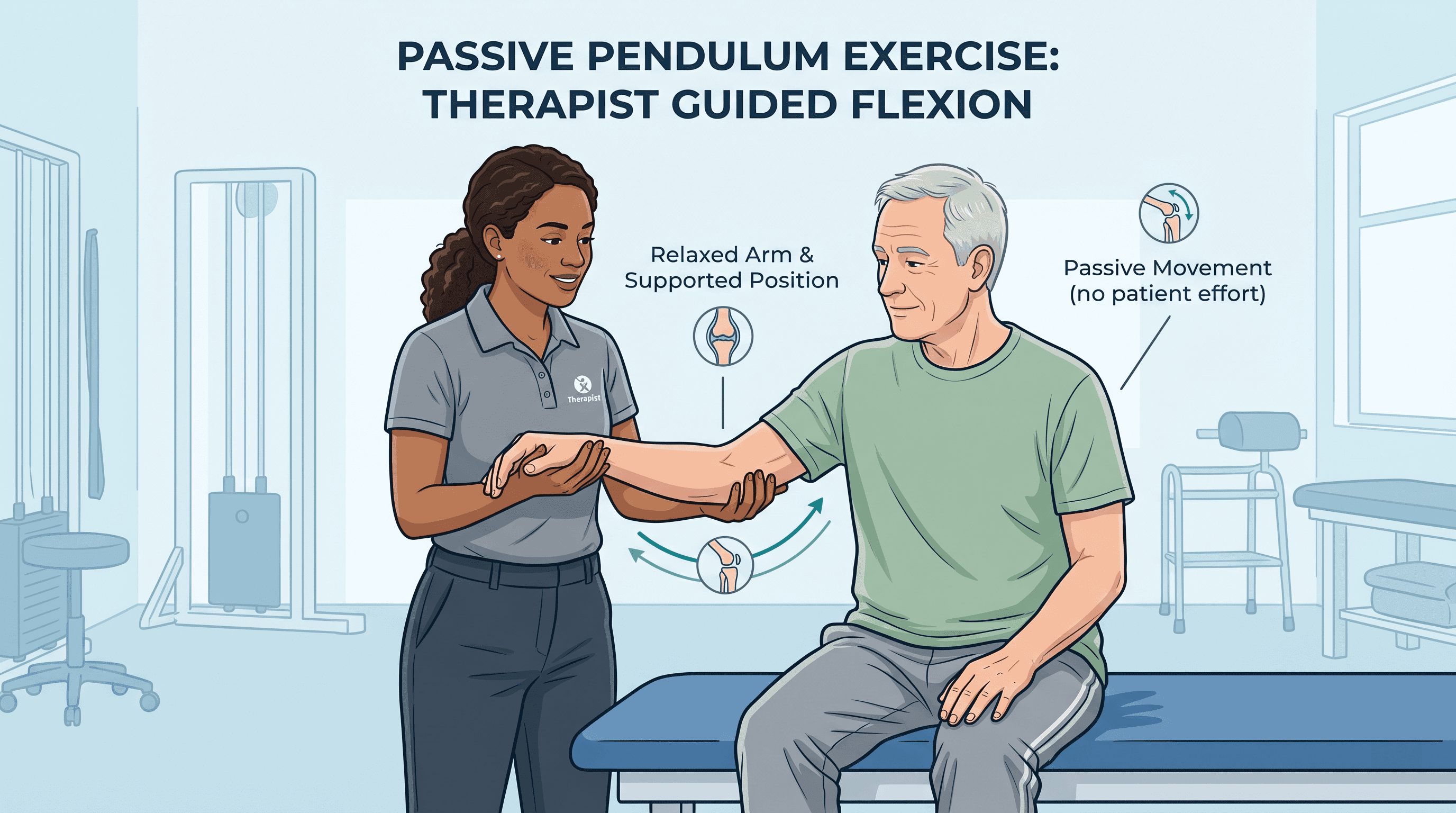
Early PT is passive range of motion work. Passive means the physical therapist moves your arm through a controlled arc while your shoulder muscles remain completely relaxed. Your job is to let it happen. The repaired tendon is under no muscular load during passive motion because the muscles attached to it are not contracting. This is what allows early movement to happen safely.
Active range of motion, where your own muscles drive the movement, typically does not begin until weeks six to twelve, depending on surgeon clearance. Active-assisted motion, where you initiate the movement and a therapist or pulley system helps complete it, usually bridges the gap between the two phases. Confusing passive and active motion is one of the most common mistakes patients make at home — reaching for something on a shelf or catching a falling object uses active contraction and can compromise a repair that passive exercises would have left fully intact.
The Early Protocol: Days 3 to 14
For patients with smaller tears and a strong repair, physical therapy begins within the first two weeks of surgery. This is often called the early or immediate mobilization protocol, and its primary objective in this phase has nothing to do with strength or function. It is entirely about preventing the shoulder from freezing.
The exercises prescribed during this window are gentle and carefully controlled. Pendulum exercises, where the patient leans forward and lets the arm hang freely, using gravity and a small rocking motion to create movement at the joint, are among the first movements introduced. Table slides, where the forearm rests on a table and slides forward with body weight providing the motion rather than the shoulder muscles, are another early staple. The physical therapist also performs hands-on passive stretching to work the joint through its range before scar tissue can organize along restricted planes.
Pain management during this phase is an active part of the session. Ice, positioning guidance, and soft tissue work around the shoulder girdle help reduce the swelling and discomfort that accompany the body's initial inflammatory response to surgery. Patients in the early protocol typically attend PT two to three times per week during this window and continue a prescribed home exercise program daily between sessions.
The Delayed Protocol: Weeks 4 to 6
Patients with massive tears, poor tendon quality, or complex repairs involving the subscapularis tendon on the front of the shoulder are often placed on a delayed mobilization protocol. This means the arm remains in a sling, and formal PT does not begin for four to six weeks after surgery.
This is not a complication or a setback. It is a deliberate clinical decision made to protect a repair that needs more time before any tension is placed on the healing tissue. Massive tears (typically defined as tears greater than 5 cm involving two or more tendons) carry a higher retear rate even under the best conditions, and the research cited above from PMC11869375 reinforces that early motion in this population elevates that risk further.
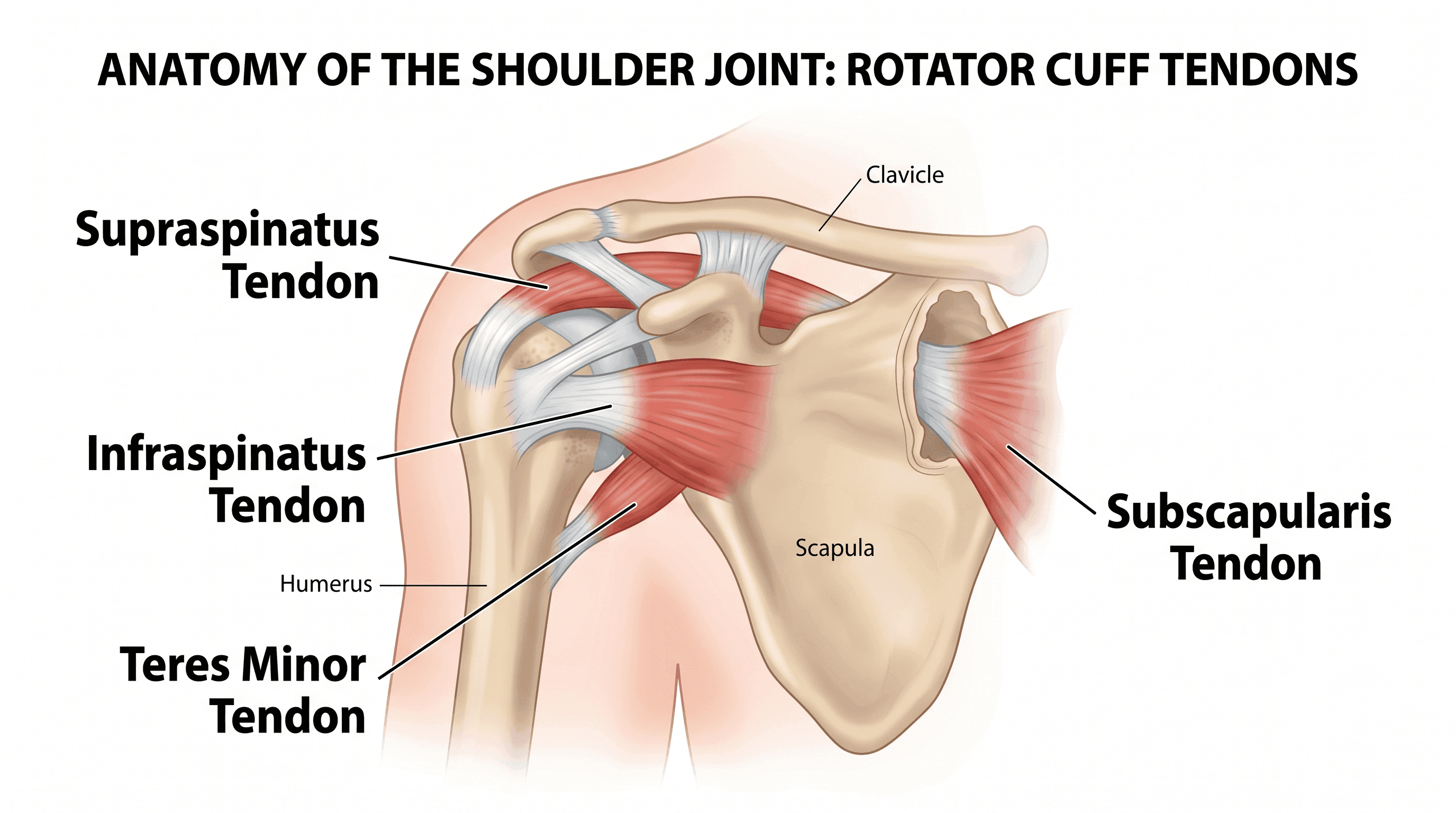
The subscapularis, the large tendon on the front of the shoulder responsible for internal rotation, requires particular caution after repair. Reaching across the body, placing the hand behind the back, or any external rotation beyond a safe arc can stress this repair before the tendon-to-bone interface has sufficient strength. Surgeons who repair subscapularis tears often impose strict positional restrictions for the first four to six weeks, and PT protocols in this group are structured around those restrictions from the very first appointment.
Patients in the delayed protocol are not doing nothing during those initial weeks. Grip squeezes, elbow flexion and extension, and wrist movements keep circulation moving and prevent stiffness in the parts of the arm that were not operated on. This matters more than it sounds.
What to Expect at Your Very First PT Appointment
For many patients, the anticipation of the first PT session is its own source of anxiety. Walking in without knowing what will happen makes the experience harder than it needs to be.
The first appointment is primarily an evaluation. The physical therapist will review your surgical report or operative notes if available, conduct a pain assessment, and establish a baseline for where your shoulder is today in terms of range and sensitivity. They will not push through significant pain on day one. The goal is information, not progress.
The therapist will likely remove the sling and gently assess passive range of motion in several planes, noting how far the arm moves comfortably and where resistance begins. Soft tissue work, including gentle massage around the shoulder, upper trapezius, and neck, often follows. This addresses the compensatory tension that builds from weeks of holding the arm protected close to the body.
You will leave the first appointment with a home exercise program. It will feel almost too simple. For patients on the early protocol, this typically means pendulum exercises two to three times per day, each lasting two to three minutes. The therapist will show you exactly how to perform them and, equally important, what not to do between sessions.
The Danger of Going Rogue at Home
Recovery from rotator cuff surgery requires a specific kind of patience that does not come naturally to most people. The shoulder begins feeling better before the repair is ready, and that gap between perceived improvement and actual tissue maturity is where the majority of home setbacks occur.
The most common mistake is using the arm under active muscle power before the surgeon has cleared it. Reaching out to stop a door from swinging, lifting a glass of water with the repaired arm at shoulder height, or supporting weight through a straightened arm, all of these movements fire the rotator cuff muscles and load the repair in ways that passive motion never does. A tendon-to-bone junction at three weeks post-surgery has not yet developed the collagen cross-linking it needs to tolerate that load.
Skipping the prescribed pendulum exercises is the other common error, and it pulls in the opposite direction. Patients who find the exercises uncomfortable, or who interpret rest as the safest strategy, are unknowingly allowing scar tissue to accumulate unchecked. A 2020 study in BMC Musculoskeletal Disorders found that adherence to prescribed home exercise protocols was one of the stronger predictors of shoulder range of motion outcomes at six months post-repair.
If something feels wrong, such as sudden sharp pain, a popping sensation, or a rapid loss of motion that had been improving, contact the surgeon's office before the next scheduled PT session.
How to Tell If PT Is Too Aggressive
Physical therapy after rotator cuff surgery is supposed to feel like work. But not all shoulder discomfort during PT is equal, and knowing the difference protects the repair and prevents unnecessary setbacks.
A dull, achy stretch across the front, back, or top of the shoulder during a passive range of motion session is typical. This is the sensation of stiff scar tissue being gradually lengthened. It fades within an hour or two after the session ends. Soreness the following morning that eases once the shoulder warms up is also within the normal range for this stage of recovery.
The warning signs are qualitatively different. Sharp, localized pain at a specific point in the arc of motion, particularly if it appeared suddenly rather than building gradually, warrants attention. Pain that does not resolve within 24 hours of a session is a signal to tell the therapist before the next appointment begins, not after. A significant increase in swelling, a warm or red surgical site, or any fever alongside shoulder symptoms should prompt a call to the surgeon's office rather than a return to PT.
A well-trained physical therapist will ask about post-session symptoms at every appointment. Honest reporting is part of the treatment. The protocol adjusts based on how the shoulder responds, and that adjustment loop only works if the patient communicates clearly.
If you are uncertain whether your current PT program is appropriate for your specific repair, consulting with a specialist is a straightforward next step. Find a board-certified orthopedic specialist or physical therapist through Momentary Lab's provider directory to review your post-operative protocol and confirm it matches your surgical findings.
Frequently Asked Questions
When should I stop physical therapy after rotator cuff surgery?
Most patients complete formal PT between four and six months after surgery, though the full recovery window extends to nine to twelve months for larger tears or physically demanding occupations. The decision to discharge from PT is typically based on functional goals, such as returning to overhead work, sport, or specific daily activities, rather than a fixed calendar date. Some patients continue a home maintenance program indefinitely to preserve strength and range of motion.
What are the first PT exercises after rotator cuff surgery?
The first exercises introduced are pendulum exercises and therapist-assisted passive stretching. Pendulum work involves leaning forward and letting the arm hang, using gentle body momentum to create small circular or forward-backward arcs at the shoulder joint. These are passive movements, meaning the shoulder muscles do not contract. Table slides and passive pulley-assisted forward flexion are also common early additions, always within the range and restrictions defined by the surgeon.
How painful is physical therapy after rotator cuff surgery?
Early PT should produce mild to moderate stretch discomfort, not sharp or stabbing pain. The sensation of tight scar tissue being lengthened is a normal part of the process and generally resolves within a day of the session. Pain that is sharp, localized to a specific point, or that does not settle within 24 hours should be reported to the therapist and potentially to the surgeon. A well-designed PT program progresses gradually and should not repeatedly provoke significant pain.
How long does it take for tendons to reattach to bone after rotator cuff surgery?
Tendon-to-bone healing is a biological process that occurs in overlapping stages. Initial tissue bridging begins within the first few weeks, but the repair site does not reach meaningful mechanical strength until approximately six weeks post-surgery, according to protocols referenced by major orthopedic institutions including the University of Iowa MOON program. Collagen remodeling continues for up to twelve months, which is why return to heavy overhead activity is typically restricted well beyond when the shoulder feels normal. A doctor can advise on individual cases based on intraoperative findings.
References
- Hu et al., BMC Musculoskeletal Disorders (2023) — Meta-analysis on early versus delayed mobilization protocols for rotator cuff repair; cited for tear size thresholds and retear risk data.
- University of Iowa MOON Post-Operative Rotator Cuff Repair Immediate Therapy Protocol (2024) — Clinical protocol document; cited for same-day and early passive motion clearance criteria.
- BMC Musculoskeletal Disorders (2020), PMC7714306 — Study on home exercise program adherence and post-operative range of motion outcomes.



