
At a Glance
| Topic | Key Facts |
|---|---|
| Primary cause of early tightness | Post-operative swelling (joint effusion) |
| Primary cause of late tightness | Scar tissue formation |
| Meniscectomy tightness timeline | Mostly resolves by weeks 4 to 6 |
| Meniscus repair tightness timeline | Full ROM typically by months 3 to 6 |
| Arthrofibrosis rate | Affects roughly 1% to 10% of knee surgeries |
| Red flag | Tightness that is getting worse, not better |
| When to escalate | Less than 90 degrees of flexion at 3 months post-op |
Why Does Your Knee Feel Tight After Meniscus Surgery? (The Short Answer)
If your knee feels like it has a rubber band wrapped around it after meniscus surgery, you are not imagining it, and you are not alone. A tight, heavy, band-like sensation is the most common complaint following any form of knee arthroscopy, reported by the large majority of patients in the first weeks after surgery.
Here is what most people are not told before going home: tightness after meniscus surgery rarely has a single cause. It is almost always a combination of joint fluid buildup, involuntary muscle guarding, disrupted nerve-muscle signaling, and the early stages of tissue repair, all happening at the same time. And critically, whether you had a meniscectomy (tissue removed) or a meniscus repair (tissue stitched back together) changes everything about what to expect and when.
This guide walks through the real causes, the week-by-week timeline, what relief actually looks like, and the warning signs worth bringing to your surgeon.
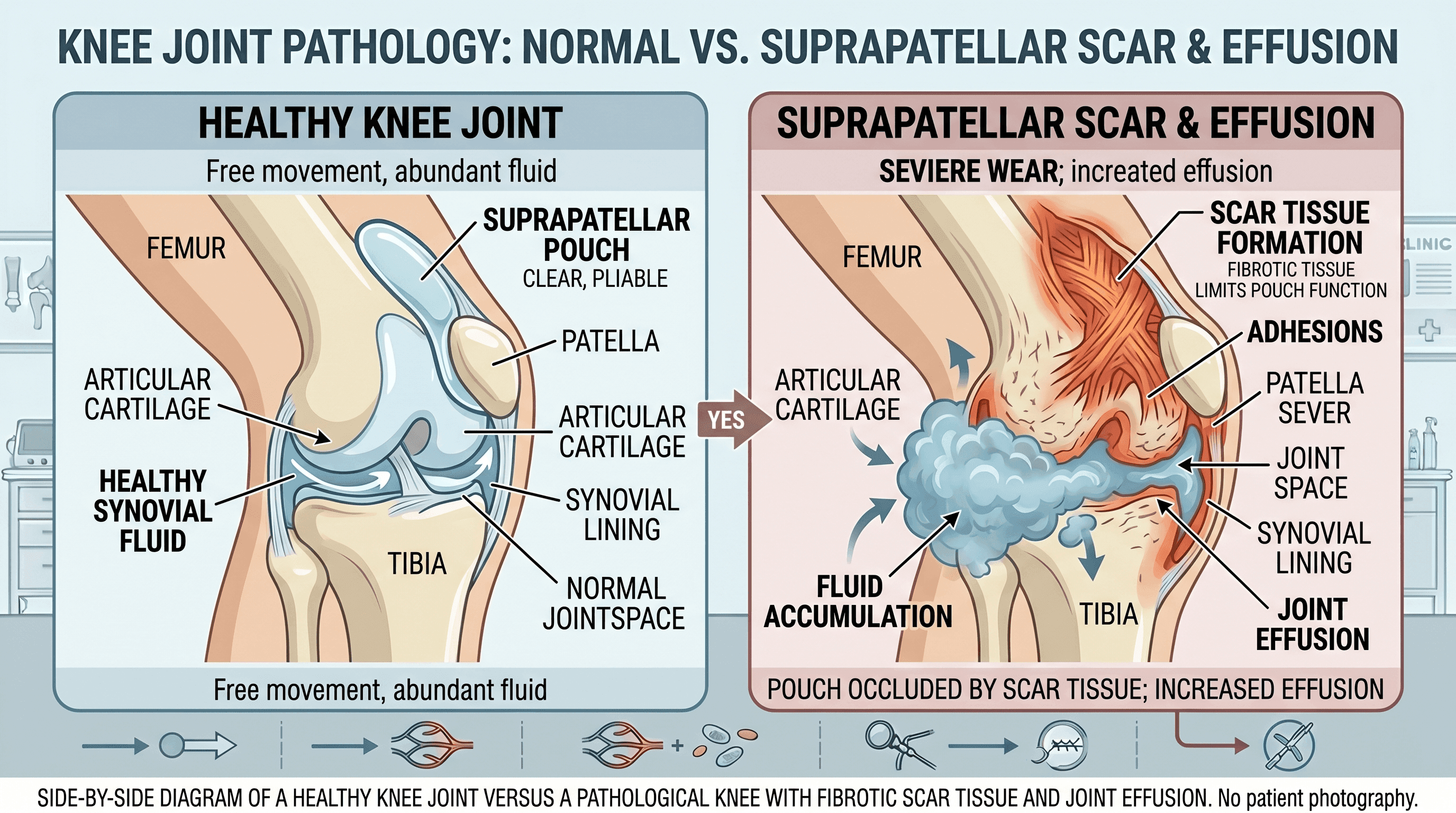
Swelling (Effusion) vs. Scar Tissue: What Is Actually Causing the Restriction?
The tightness in the first two weeks after meniscus surgery and the tightness at three months feel similar, but they are driven by completely different processes. Treating one as if it were the other is one of the most common recovery mistakes.
Post-Operative Swelling and Why It Persists Longer Than You Think
In the first days after surgery, the knee joint fills with fluid as part of the normal inflammatory response. This is called joint effusion, and it is the body doing exactly what it is supposed to do. The problem is that this fluid physically compresses the joint capsule, making full bending and straightening feel blocked.
What most patients are not warned about is that internal swelling can restrict motion for three to six months even when the knee looks completely normal from the outside. Visible swelling (the puffy, warm appearance) may clear up in two to four weeks. But internal joint fluid, which does not show up on the surface, continues to limit range of motion long after. Research published in PMC confirms that post-operative effusion is a primary driver of early functional limitation after knee arthroscopy.
Scar Tissue and Arthrofibrosis: When Healing Goes Too Far
As swelling begins to decrease, a different source of tightness can take over: scar tissue. The surgical trauma causes the body to lay down fibrous tissue as part of the healing process. In most patients, this is temporary and manageable. But in a meaningful subset, the process becomes excessive.
Arthrofibrosis is the term for pathological scar tissue formation inside the knee joint. Unlike normal post-surgical stiffness, arthrofibrosis does not gradually improve. It feels like a progressive hardening, a mechanical stop that gets tighter rather than looser over time. Patients often describe it as "my knee just won't go any further" rather than "my knee is sore when I push it."
According to research in the Journal of Orthopaedic Surgery and Research, clinically significant arthrofibrosis affects an estimated 1% to 10% of patients following knee surgery, with inadequate early mobilization being one of the most preventable contributing factors.
The distinction that matters: normal tightness gradually loosens with movement and time. Arthrofibrosis feels hard, does not respond to stretching, and may actually feel worse after activity rather than better.
The 4 Real Causes of Post-Surgery Knee Tightness
Quad Inhibition and Patellar Tracking Issues
This is the cause almost no one talks about, and it is one of the most clinically significant contributors to early tightness.
When swelling is present inside the knee joint, the nervous system reflexively shuts down the quadriceps muscle. This is called arthrogenic muscle inhibition, and it is an involuntary protective response. The quad cannot fire properly, which means the knee cannot fully extend. That loss of terminal extension feels, from the inside, exactly like joint tightness, but it is actually a neurological signaling problem, not a mechanical one.
Layered on top of this, the kneecap (patella) can begin to track poorly when the quad is inhibited. Poor patellar tracking adds a mechanical restriction that compounds the feeling of stiffness. Research published in PMC identifies arthrogenic muscle inhibition as a well-established barrier to recovery after knee surgery, one that cannot be solved by simply pushing through the pain.
The good news is that quad sets (described in the physical therapy section below) directly address this, and many patients notice an immediate change in how the knee feels once the quad begins firing again.
Muscle Guarding: Your Knee's Protective Reflex
Separate from quad inhibition, the muscles surrounding the knee, particularly the hamstrings, the IT band, and the hip flexors, involuntarily contract to brace the joint after surgery. This is called muscle guarding, and it is a subconscious protective reflex rather than a conscious decision.
The result is that even when the joint itself has adequate room to move, the surrounding musculature is actively resisting that movement. Patients often feel this as tightness behind the knee (hamstrings) or along the outer thigh (IT band) rather than inside the joint. Addressing muscle guarding is a key reason physical therapy works on the entire kinetic chain, not just the surgical site.
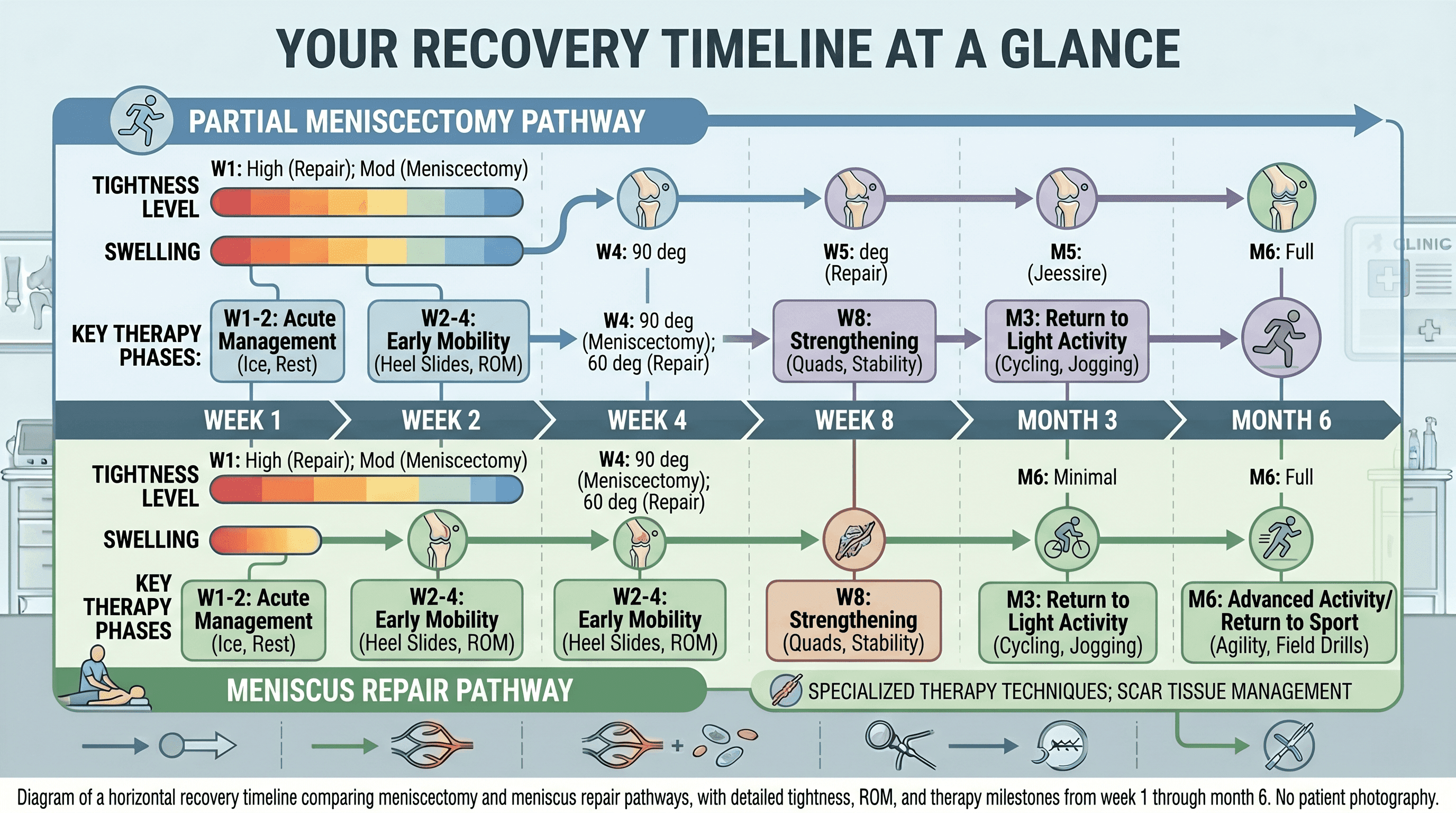
Meniscectomy vs. Meniscus Repair: Your Tightness Timeline Is Different
This is the section most recovery guides skip entirely, and skipping it leads to unnecessary anxiety for repair patients and complacency in meniscectomy patients.
The two surgeries have different healing biology, which produces different tightness timelines.
| Factor | Meniscectomy | Meniscus Repair |
|---|---|---|
| What was done | Damaged tissue removed | Tissue stitched back together |
| Weight-bearing | Often immediate or within days | Restricted for 4 to 6 weeks |
| ROM restrictions | Minimal; full ROM encouraged early | Capped at 0 to 90 degrees for weeks 1 to 6 |
| Tightness peak | Days 3 to 7 post-op | Weeks 2 to 4 (due to immobilization) |
| Tightness resolution | Largely resolved by weeks 4 to 6 | Full ROM typically by months 3 to 6 |
| Driving factor | Swelling and muscle guarding | Protocol restrictions plus swelling |
In a meniscectomy, no tissue needs to grow back together. The goal from day one is motion. Tightness resolves relatively quickly because rehabilitation can begin aggressively within the first week.
In a meniscus repair, the stitched tissue must heal before being stressed. This requires controlled immobilization and graduated weight-bearing, which means the knee is intentionally kept in a limited range of motion for weeks. The tightness patients feel at weeks three and four after a repair is partly a consequence of this necessary restriction. It is not a sign that something has gone wrong; it is a sign that the protocol is being followed.
Understanding which surgery you had is the single most important factor in calibrating your expectations.
Is Your Tightness Normal? Week-by-Week Milestones
This is the most common question on orthopedic forums, and most answers are frustratingly vague. Here is a concrete timeline based on clinical rehabilitation standards.
Week 1 to 2 Significant tightness is expected and normal for both surgery types. The knee may not bend past 90 degrees, and full extension may feel blocked. Swelling is at its peak. Meniscectomy patients should already be working on heel slides and quad sets. Repair patients are typically in a brace with motion limited to 0 to 60 degrees.
Week 3 to 4 Meniscectomy patients should be approaching 90 to 110 degrees of flexion. If bending is still significantly below 90 degrees with effort by the end of week 4, raise this with your physical therapist. Repair patients remain in a restricted protocol but should be seeing gradual improvement within their allowed range.
Months 2 to 3 Meniscectomy patients should have near-full or full range of motion by month 2. Residual tightness at this stage typically reflects ongoing muscle guarding or mild effusion rather than significant scar tissue. Repair patients are typically progressing toward 90 to 120 degrees and beginning partial weight-bearing activities.
Month 4 to 6 Repair patients targeting full ROM should reach it by month 4 to 6 under a standard rehabilitation protocol. For meniscectomy patients still reporting meaningful tightness at this stage, a clinical reassessment is warranted.
6 Months and Beyond Persistent, worsening tightness at six months, regardless of surgery type, is not a normal part of recovery. This is the threshold at which a conversation about escalation options (covered below) is appropriate.
Physical Therapy Interventions to Break Through the Stiffness
Physical therapy is the primary treatment for post-surgical knee tightness, and the specific exercises matter as much as showing up.
Phase 1 (Days 1 to 14): Swelling Control First
Before range of motion can improve, swelling must be addressed. The RICE protocol (rest, ice, compression, elevation) remains the foundation. Keeping the knee elevated above heart level for the first 72 hours reduces fluid accumulation significantly.
Modern cryotherapy compression devices, such as the Game Ready system, deliver simultaneous cold and intermittent compression and are more effective than a standard ice bag at reducing early post-operative effusion. Anti-inflammatory medications taken as directed by your surgeon also reduce joint fluid during this window. Do not skip this phase in the rush to start moving. Less swelling means less inhibition of the quad, which means faster progress in phase 2.
Phase 2 (Weeks 2 to 6): Gentle Range-of-Motion Exercises
Once swelling is controlled, the focus shifts to restoring motion without stressing healing tissue.
Heel slides involve lying on your back, slowly sliding the heel toward the buttock, holding for three to five seconds, and returning. This is the foundational ROM exercise for the early phase and can be done multiple times daily. Quad sets involve tightening the quadriceps while the leg is straight, pressing the back of the knee toward the floor, holding for five seconds, and releasing. This directly addresses arthrogenic muscle inhibition.
Prone passive flexion involves lying face-down and allowing gravity to gently bend the knee, with a light ankle weight added as tolerance improves. Dangle stretches (sitting on the edge of a bed and letting gravity flex the knee) use body weight to gain flexion gently. Patellar mobilizations, performed by a physical therapist, involve manually moving the kneecap in all four directions to prevent scar tissue from restricting its glide.
For repair patients in weeks 2 to 6: ROM is typically restricted to 0 to 90 degrees per protocol. Do not exceed this range even if it feels comfortable to do so. Overstressing the repair during this window can compromise the fixation.
Phase 3 (Weeks 6 and Beyond): Strengthening and Full Mobility
Once adequate ROM is established, the focus shifts to rebuilding strength, which further reduces guarding and tightness. Straight leg raises, hamstring curls, and step-ups are standard progressions.
One increasingly used technique for repair patients is blood flow restriction (BFR) training. BFR uses a pneumatic cuff to partially occlude venous return during low-load exercise, allowing meaningful muscle activation at loads that do not stress healing tissue. Research in the PMC database supports BFR as a method for maintaining quad strength during the restricted early phases of repair recovery.
A stationary bike is also a valuable tool at this stage. The cyclical motion promotes synovial fluid distribution, reduces stiffness, and builds quad endurance simultaneously. Begin with minimal resistance and prioritize the full pedal revolution as a ROM exercise before adding load.
Regarding massage: soft tissue massage to the thigh musculature and along the IT band is appropriate and often helpful from weeks 4 to 6 onward. Direct massage over the surgical incision sites should wait until cleared by your surgeon, typically when incisions are fully healed and no longer tender.
Why Your Knee Feels Tighter in the Morning (and What to Do)
This catches nearly every post-surgical patient off guard. Waking up to a significantly stiffer knee than you had when you went to sleep is not a sign of regression.
During sleep, synovial fluid, the joint's natural lubricant, pools and becomes less evenly distributed. Circulation slows, tissue cools, and the muscles that were gradually relaxing all day return to a guarded state overnight. The result is that the first steps of the morning feel like starting from scratch.
The fix is a short pre-activity warm-up before standing or walking. Five minutes of heel slides in bed, gentle ankle pumps, and quad sets while still lying down will redistribute synovial fluid and signal the muscles to release their overnight guarding. Most patients find the morning stiffness reduces significantly within 10 to 15 minutes once they begin moving.
At-Home Strategies to Relieve a Tight Knee
Physical therapy addresses the structural and neuromuscular drivers of tightness. At home, the day-to-day management comes down to knowing which tool to use at which stage.
In the first two weeks, ice is the correct choice. Cold reduces metabolic activity in the joint, decreases effusion, and blunts pain. Apply for 15 to 20 minutes at a time, with at least 45 minutes between applications, and always use a cloth barrier between ice and skin.
From weeks three to four onward, as acute swelling decreases, heat becomes appropriate for muscle-driven tightness. A warm compress applied to the thigh and calf muscles for 10 to 15 minutes before exercises helps release muscle guarding and improves tissue extensibility. Do not apply heat directly over the incision sites while they are still healing.
Elevation remains useful beyond the first two weeks when the knee feels heavy or swollen at end-of-day, particularly after longer periods of walking or standing. Lying flat with the leg elevated on two pillows (ankle above knee, knee above hip) drains residual fluid effectively.
Compression wraps or sleeves provide proprioceptive feedback that can reduce guarding during activity, though they should not be so tight as to impede circulation.
Warning Signs: When Tightness Signals a Complication
Most post-surgical tightness follows a predictable, improving course. But there are patterns that warrant an immediate call to your surgeon, not a wait-and-see approach.
Signs of arthrofibrosis: The knee is not gradually getting looser. Stiffness feels mechanical and hard rather than tight and sore. Range of motion is decreasing or has plateaued significantly below expected benchmarks. This is the "tight and getting worse" pattern rather than "tight and slowly improving."
Signs of infection: Increasing warmth, redness, or swelling around the incision sites. Discharge from the wound. Fever above 100.4 degrees Fahrenheit. Pain that is escalating rather than following the expected improvement curve.
Signs of deep vein thrombosis (DVT): Calf pain, calf warmth, or unexplained swelling in the lower leg. DVT is a known complication following orthopedic procedures and requires urgent evaluation. If you have sudden calf tightness and swelling after meniscus surgery, go to an emergency department rather than waiting for a scheduled appointment.
Signs of failed repair: Locking (the knee gets stuck mid-motion and will not complete the movement), giving way (the joint buckles unpredictably under weight), or pain that was improving and has suddenly worsened following a specific activity or incident.
If you are unsure whether what you are experiencing falls into normal variation or a potential complication, connecting with a qualified orthopedic specialist is the right step. You can find a doctor through Momentary Lab's physician directory to locate a specialist near you.
When Conservative Treatment Is Not Enough: Escalation Options
For most patients, physical therapy and home management are sufficient. But when tightness persists beyond expected timelines or stops responding to conservative care, there is a clear escalation pathway.
Intensified physical therapy is the first step when progress stalls. This typically means increasing session frequency, adding manual therapy techniques such as joint mobilizations and instrument-assisted soft tissue mobilization, and reassessing the home exercise program for gaps.
Corticosteroid injection can be appropriate when persistent joint effusion is confirmed to be driving ongoing restriction. A steroid injection into the joint reduces inflammation and can break a cycle of swelling-induced inhibition. This is typically considered at six to twelve weeks if swelling remains a dominant factor.
Manipulation Under Anesthesia (MUA) is a procedure used when significant loss of range of motion persists at three to six months post-op, typically defined as less than 90 degrees of flexion. Under general or regional anesthesia, the surgeon manually moves the knee through its full range of motion to break up scar tissue adhesions. Recovery following MUA requires immediate aggressive physical therapy to maintain the gains achieved. Most patients see meaningful improvement, though repeat MUA is occasionally necessary.
Arthroscopic scar tissue removal (lysis of adhesions) is the surgical option reserved for confirmed arthrofibrosis that has not responded to MUA. The surgeon re-enters the joint to physically remove scar tissue under direct visualization. This carries its own recovery period and the risk of re-formation, which is why it is reserved for cases that have exhausted less invasive options.
Knowing these options exists empowers you to have a specific, informed conversation with your surgeon if conservative management is not delivering results.
Frequently Asked Questions
How do I loosen my knee after meniscus surgery?
The most effective approach combines swelling control with targeted movement. In the first two weeks, prioritize ice, elevation, and compression to bring fluid levels down. From there, heel slides, quad sets, and patellar mobilizations performed daily are the core tools for restoring motion. A stationary bike (once cleared by your surgeon or PT) is one of the most efficient tools for improving both ROM and circulation simultaneously. Avoid long periods of static positioning, as the knee stiffens quickly when it is not being moved through its range.
How long is the knee stiff after meniscus surgery?
This depends heavily on which surgery you had. After a meniscectomy, most patients see significant stiffness resolve by weeks four to six. After a meniscus repair, meaningful stiffness often persists through months two to three due to the more protective rehabilitation protocol, with full ROM typically restored by months three to six. Stiffness that has not meaningfully improved by the three-month mark, regardless of surgery type, should prompt a reassessment with your surgeon or physical therapist.
Why does my knee still hurt five months after meniscus surgery?
Pain and tightness at five months can reflect several things: residual effusion, scar tissue, inadequate quad strength leading to altered mechanics, or in some cases re-injury to the repair. It can also reflect a co-existing condition such as underlying cartilage damage that was present before surgery and was not the primary surgical target. Five months is the outer boundary of what most orthopedic surgeons would call "still within normal healing variation" for a repair. A reassessment appointment, potentially with imaging, is appropriate at this stage to rule out structural issues.
What does arthrofibrosis feel like vs. normal tightness?
Normal post-surgical tightness feels like soreness at the end of range, as though the joint is reluctant but moveable. It gradually improves with consistent work. Arthrofibrosis feels mechanical rather than painful, as though there is a hard stop before the normal end of range. It does not respond to gentle stretching the way normal stiffness does, and it often feels worse after activity rather than better. If your knee feels like it physically cannot go any further regardless of how relaxed you are, rather than that it is sore when you push it, that pattern warrants evaluation.
Can I massage my knee after meniscus surgery?
Yes, with appropriate timing and location. Soft tissue massage to the quadriceps, hamstrings, IT band, and calf is appropriate from weeks four to six onward and can meaningfully reduce muscle guarding. Direct massage over the incision sites should wait until the incisions are fully closed, non-tender, and cleared by your surgeon, typically around the four to six-week mark. Do not perform deep pressure massage directly over the joint line without guidance from a physical therapist.
What is manipulation under anesthesia for knee stiffness?
Manipulation Under Anesthesia (MUA) is a procedure performed by an orthopedic surgeon in which the knee is moved through its full range of motion while the patient is under anesthesia, allowing the surgeon to break up scar tissue adhesions that are blocking motion. It is typically considered when a patient cannot achieve at least 90 degrees of flexion by three to six months post-operatively despite consistent physical therapy. The procedure itself takes minutes, but the recovery requires immediate and aggressive physical therapy to maintain the ROM gains. Most patients experience a meaningful improvement in motion following MUA.
References
- PMC: Post-operative effusion and functional limitation after knee arthroscopy — Cited for joint effusion as a primary driver of early functional limitation after knee arthroscopy.
- Journal of Orthopaedic Surgery and Research: Arthrofibrosis incidence and contributing factors — Cited for arthrofibrosis prevalence (1% to 10%) and role of early mobilization.
- PMC: Arthrogenic muscle inhibition and blood flow restriction training after knee surgery — Cited for arthrogenic muscle inhibition mechanism and BFR training evidence.
- PubMed: Meniscus repair outcomes and rehabilitation — Cited for context on meniscus repair recovery timelines and rehabilitation protocols.



