
At a Glance
| Topic | Key Facts |
|---|---|
| US healthcare spending (2023) | $4.9 trillion, 17.6% of GDP |
| Projected annual AI savings | $200B to $360B (McKinsey/Harvard) |
| Long-range AI savings potential | $400B to $1.5T by 2050 (Morgan Stanley) |
| Enterprise AI implementation cost | $500K to $5M+ |
| Administrative waste share of spending | ~25% of total healthcare expenditure |
| Hospital readmission annual cost | $26B+ in Medicare penalties and avoidable care |
| Ambient scribe market size (2025) | ~$600M and growing |
| AI project failure rate | Approximately 80% do not meet expected outcomes |
The Short Answer: Trading Upfront Investment for Long-Term Value
AI in healthcare is not a cost-cutter in the way a budget freeze is. It is more like a infrastructure investment that targets the inefficiencies baked so deeply into the system that clinicians have stopped seeing them.
Roughly 25% of all US healthcare spending goes to administrative tasks, according to a study published in JAMA. That is not care. That is paperwork, prior authorizations, billing disputes, coding errors, and scheduling friction. AI targets this layer with specific and measurable force.
The ai healthcare cost conversation has two sides that most articles refuse to hold at the same time: the savings potential is genuinely large, and the implementation costs are genuinely high. Getting value out of AI in medicine requires understanding both numbers clearly before signing any contract.
This guide covers the real savings broken down by category, the realistic price ranges for deployment in 2026, and the risks that do not appear in vendor pitch decks.
Slashing Administrative and Billing Overhead
The fastest, most proven wins from AI in healthcare come from the administrative layer, not the clinical one.
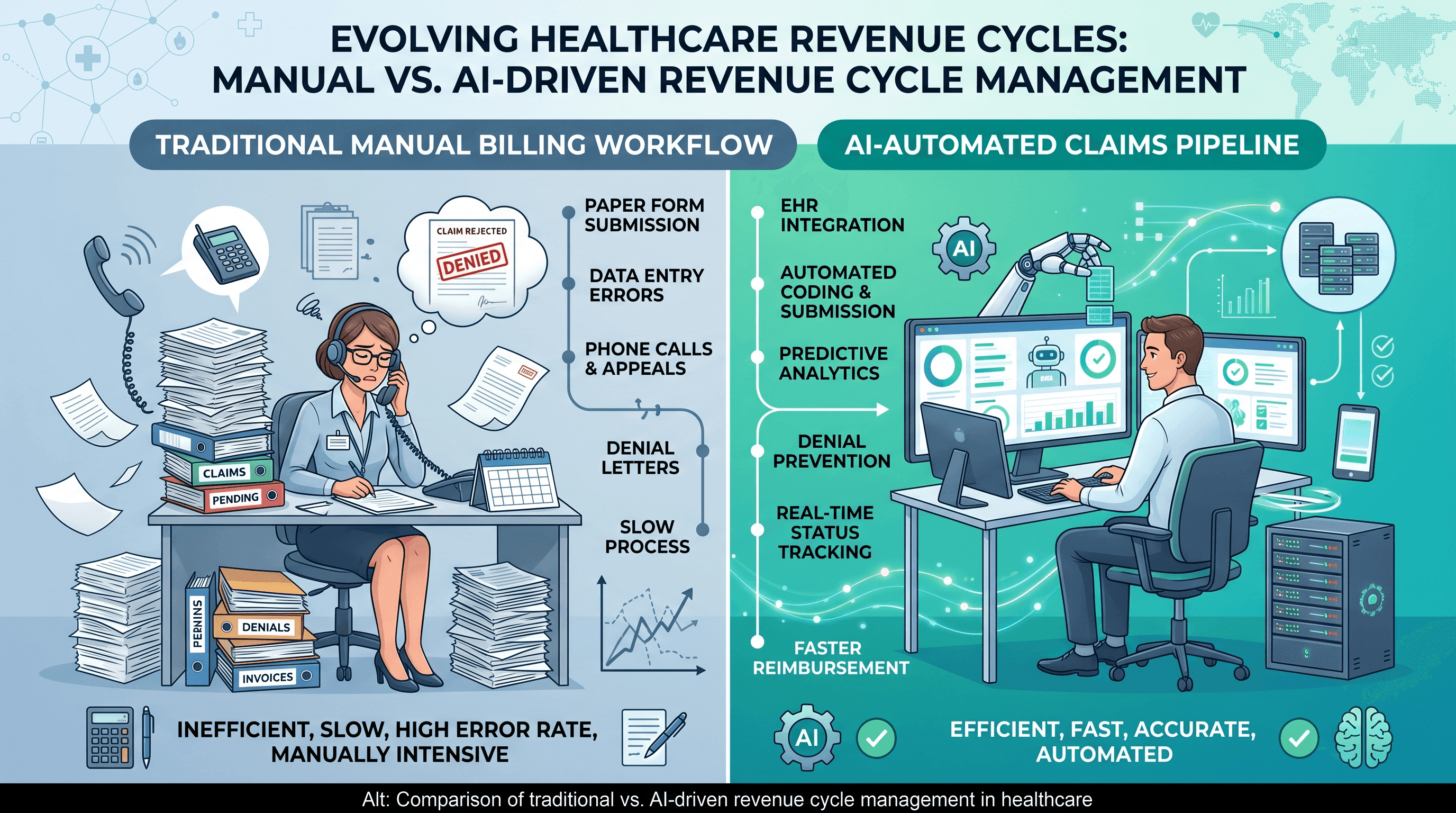
The US healthcare system processes billions of insurance claims per year, and billing errors alone cost providers an estimated $935 million annually, according to data from the American Hospital Association. AI-driven Revenue Cycle Management (RCM) software reads clinical documentation, auto-populates billing codes, checks for payer-specific rules, and flags likely denials before a claim is ever submitted.
Prior authorization is a specific subset of billing overhead that has become a full industry problem. Physicians report spending an average of nearly two full working days per week on prior authorization requests, according to the American Medical Association. AI agents can now submit, track, and escalate prior auth requests autonomously, with some health systems reporting a 70% reduction in manual processing time after deployment.
Claims fraud is another category where AI delivers measurable returns. A 2024 Wall Street Journal investigation found Medicare paid approximately $50 billion for services tied to nonexistent or fraudulent treatments. Machine learning systems trained on historical claims data can flag anomalous billing patterns in real time, something that manual auditing cannot do at scale.
For health insurers and large payers, the combined opportunity from prior auth automation, fraud detection, and claims processing optimization is estimated at $80B to $110B annually, based on projections cited in the McKinsey Global Institute analysis on AI in healthcare.
"Administrative complexity is the single largest driver of waste in US healthcare, accounting for roughly $265 billion in unnecessary spending annually."
New England Journal of Medicine
Reducing Hospital Readmissions via Predictive Care
Hospital readmissions represent one of the most expensive categories of preventable healthcare spending, and AI is making meaningful progress on this front.
When a patient is discharged and returns to the hospital within 30 days, the Centers for Medicare and Medicaid Services (CMS) penalizes the hospital under the Hospital Readmissions Reduction Program. The total financial exposure across the US hospital system runs into the tens of billions annually. AI changes the calculus by predicting which patients are at high risk of readmission before they leave the building.
Predictive models trained on electronic health record (EHR) data, vitals, lab values, and social determinants of health can score each patient's readmission risk at discharge. High-risk patients can then be routed into intensive follow-up protocols: automated check-in calls, remote monitoring, or earlier outpatient appointments. A study in JAMA Internal Medicine found that AI-assisted discharge planning reduced 30-day readmission rates by 20% to 30% in participating health systems.
The same predictive infrastructure applies inside the ICU. Early warning systems powered by machine learning monitor streaming vital signs and lab data, alerting care teams to patient deterioration up to six hours before clinical signs become obvious to bedside nurses. Earlier intervention means shorter ICU stays, fewer transfers to higher-acuity care, and lower per-encounter costs.
For hospitals and large health systems collectively, the estimated savings from clinical operations optimization, ambient AI documentation, and readmission reduction land between $60B and $120B per year, according to projections from McKinsey and Harvard research.
The Cost of Triage: AI vs. Emergency Rooms
One of the largest patient-side savings opportunities in the US healthcare system sits at the front door of the emergency room.
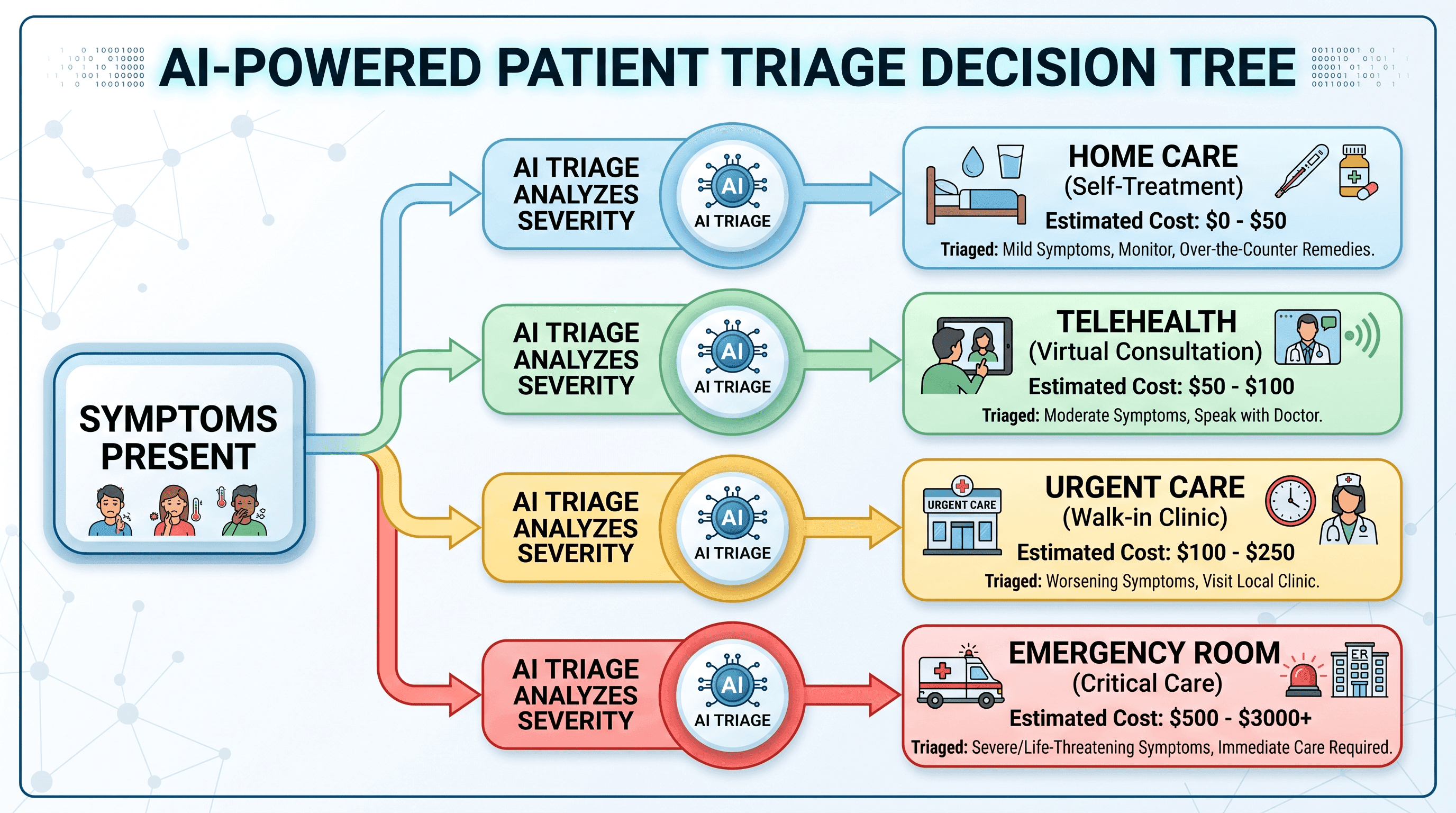
The average ER visit in the United States costs between $1,500 and $3,000 when accounting for facility fees, labs, and imaging, according to data from the Healthcare Cost Institute. A significant portion of those visits, estimated at 30% to 40% by the American College of Emergency Physicians, involve conditions that could safely be addressed through a telehealth visit, urgent care clinic, or self-care guidance.
AI-powered symptom checkers and triage tools sit at that decision point. They ask structured questions, assess symptom severity against clinical algorithms, and direct patients to the appropriate level of care: a $50 telehealth visit instead of a $2,000 ER encounter. For patients without insurance or with high-deductible plans, that difference is not marginal. It is the difference between seeking care and avoiding it entirely.
Insurers benefit proportionally. Each avoided ER visit for a non-emergency condition removes a high-cost claim from the system. At scale, AI triage tools embedded in insurance apps, employer wellness platforms, and health system patient portals represent a category of savings that is hard to model precisely but structurally significant.
Physician groups and outpatient practices also benefit from AI-assisted care coordination. No-show rates in outpatient medicine cost the industry an estimated $150 billion annually, as reported by JAMA Network. AI scheduling systems that send personalized reminders, identify patients with transportation barriers, and automatically offer rescheduling options reduce no-show rates by 20% to 40% in documented pilots.
Implementation Costs: What Providers Can Expect to Pay
This is the section most AI coverage skips entirely, which is a disservice to any operator trying to make a real budget decision.
AI implementation in healthcare does not have a single price tag. Costs depend on organizational size, existing data infrastructure, the complexity of the use case, and whether a vendor is offering a preconfigured SaaS product or a custom-built enterprise solution.
SaaS subscriptions for smaller practices typically run $500 to $2,000 per provider per month for ambient documentation tools like DAX Copilot or Suki. These tools transcribe and structure clinical notes in real time, reducing documentation time by an average of 1.2 to 1.5 hours per provider per day compared to the current baseline of 4.7 hours of documentation burden cited in American Medical Association surveys. At the low end, a five-physician practice might spend $60,000 to $120,000 per year on ambient scribing software, with a realistic productivity gain that offsets that cost within 12 to 18 months.
Mid-market deployments for regional health systems or multi-specialty groups integrating AI into billing, scheduling, and care management typically run $200,000 to $800,000 in the first year, including implementation, training, and integration fees.
Enterprise AI deployments for large hospital systems or health plans, particularly those building custom clinical decision support or diagnostic imaging models, range from $500,000 to $5 million or more depending on scope. These costs include GPU infrastructure or cloud compute fees, clinical informatics staff to manage data pipelines, legal and compliance review for HIPAA and FDA regulatory requirements, and change management programs to drive clinical adoption.
Estimating Your ROI Timeline
For operators bringing AI cost-benefit data to a CFO, the general framework from McKinsey projects 200% to 400% ROI within three to five years for well-scoped AI deployments focused on high-frequency, high-volume tasks.
A simplified example: a 200-bed hospital deploying ambient scribing at $150,000 per year, serving 40 physicians, and recovering one additional patient encounter per physician per day at an average revenue of $200 per encounter would generate $2.9 million in annual revenue recovery. Net ROI in year one: approximately $2.75 million. That math does not hold for all use cases, and it assumes strong adoption, which is itself a cost to manage.
The hidden costs that most vendor proposals undercount include data readiness work (getting EHR data into FHIR-compatible formats is often a multi-month project), ongoing model maintenance as clinical guidelines update, and the staff time required to audit AI outputs for accuracy during the early deployment period.
The Risks and Hidden Costs AI Boosters Do Not Mention
No honest evaluation of ai healthcare cost can skip this section, even though most articles do.
Care cascade inflation. AI diagnostic tools, particularly in imaging, often improve sensitivity, meaning they detect more findings. More findings generate more follow-up: additional scans, biopsies, specialist referrals, and procedures. When those downstream steps confirm benign incidental findings, the net effect on total cost of care can be inflationary. A study in the New England Journal of Medicine examining expanded cancer screening programs documented this pattern clearly: better detection led to more treatment, some of which targeted cancers that would never have caused harm. AI-assisted radiology is valuable, but health systems need to model the downstream cost of incidental findings before assuming net savings.
The AI coding wars. As providers deploy AI to optimize billing codes upward (a process called upcoding), payers are deploying their own AI to detect and deny those exact patterns. The result is an arms race where both sides spend on AI without the patient seeing lower costs. Research published in AJMC has documented payers using AI to issue blanket prior auth denials for specific procedure codes, shifting the administrative burden back to providers who must then appeal with human staff.
The 80% failure rate. Approximately 80% of AI health initiatives do not achieve their expected outcomes, according to analyses of AI implementation studies cited in Frontiers in Public Health. The most common failure modes are poor data quality at the source, workflow designs that clinicians work around rather than with, and insufficient governance to catch model drift over time.
Downtime contingency costs. An AI system embedded deeply into clinical workflows creates a single point of failure. Health systems that have not planned for AI downtime scenarios, including backup workflows, staff training on manual processes, and vendor SLA guarantees, can face operational disruption that exceeds the savings the system was generating.
If any of these risks feel present in a current or planned AI deployment, connecting with a clinical informatics expert before scaling is worth the investment. For patients with questions about their own care costs or coverage options, see a doctor online through Momentary to get guidance without the overhead of an in-person visit.
Agentic AI: The 2026 Shift Changing the Cost Equation
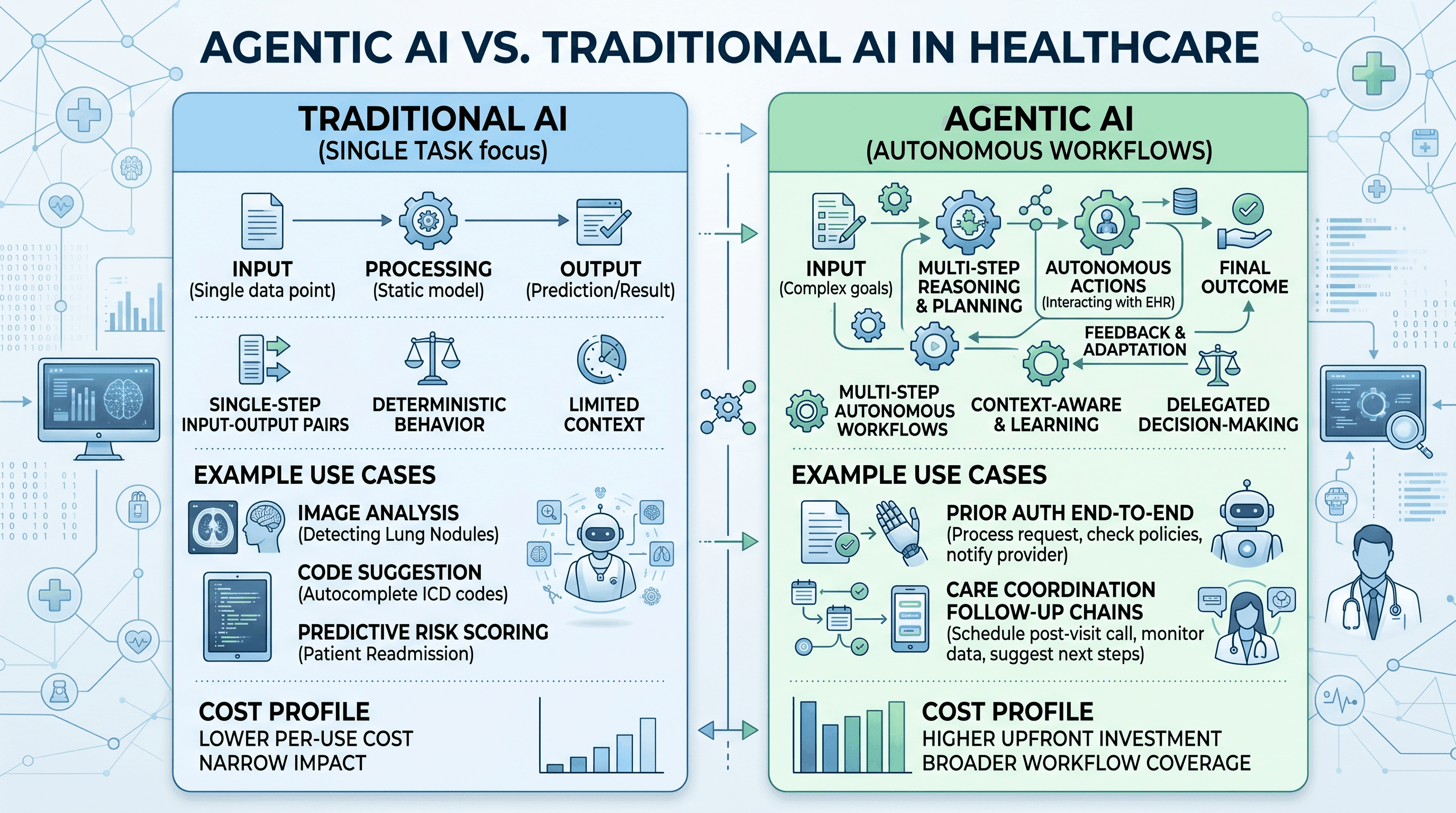
Traditional healthcare AI is task-specific. It reads an X-ray, suggests a billing code, or flags a drug interaction. Agentic AI is different in kind, not just degree.
Agentic AI refers to systems that can execute multi-step workflows autonomously, making decisions, calling external systems, and adapting to intermediate results without constant human instruction. In healthcare, this means an AI agent that receives a prior authorization request, pulls the relevant clinical documentation from the EHR, formats it to payer specifications, submits it, monitors the response, and escalates denials, all without a staff member touching the case.
The growth trajectory for agentic AI in healthcare is steep. Patient engagement agents have grown more than 20 times year-over-year as of 2025, and prior authorization agents have grown more than 10 times year-over-year, according to industry tracking from healthcare AI infrastructure firms. The ambient scribe market alone reached approximately $600 million in 2025 and is projected to grow significantly through 2027.
The cost profile for agentic AI differs from traditional AI in a way that matters for budget planning. Because agentic systems handle end-to-end workflows rather than single tasks, the ROI calculation changes. Labor displacement is more complete per use case, but implementation complexity is higher and the failure modes are more consequential when they occur.
Barriers to Adoption: Why Most Hospitals Have Not Scaled AI Yet
If AI savings are this clear, why are so few health systems realizing them at scale?
The answer has several layers, and none of them are simple. Legacy EHR fragmentation is the most structurally significant barrier. Most health systems operate across multiple EHR platforms with different data standards, and only a fraction of that data is in the FHIR-compatible format that modern AI systems require. Getting data ready for AI can cost as much as the AI deployment itself.
Only 16% of healthcare organizations have a formal AI governance framework in place, according to surveys of health IT leaders. Without governance, models drift, outputs go unchecked, and the liability exposure for AI-assisted clinical decisions becomes unclear and unmanaged.
Fee-for-service payment models create misaligned incentives. AI that prevents a hospitalization saves money for payers and patients but reduces revenue for the health system that deployed it. Until value-based care arrangements become the dominant payment model, AI investments that reduce utilization face an internal financial headwind inside the organizations that would benefit most from them.
Staff resistance is real and rational. Clinicians who spent a decade learning a documentation workflow do not automatically trust a system that was trained on someone else's data. Change management, clinical champion programs, and transparent model performance reporting are the difference between AI adoption rates of 30% and 90%.
Data readiness, as noted in the implementation cost section, is consistently underestimated. A study in PMC/NLM found that data preparation and cleaning consumed 60% to 80% of total project time in healthcare AI implementations, far exceeding the time spent on model development itself.
A Practical Roadmap: How to Start Capturing Savings Now
The organizations capturing AI savings fastest in 2026 are not the ones who tried to transform everything at once.
Start with administrative automation. Ambient scribing, prior auth automation, and claims scrubbing all have high ROI, low clinical risk, and short implementation timelines compared to clinical AI. For a small practice, ambient scribing alone can pay back its cost within a year while improving physician satisfaction, which has its own downstream retention value.
Before signing any AI contract, audit data readiness. Ask the vendor specifically what EHR integrations are supported, what data cleaning is included in the implementation fee, and what happens when the source EHR is upgraded. Surprises in the integration layer are the most common cause of cost overruns.
Define ROI metrics before deployment, not after. Specific, measurable targets for documentation time saved, claim denial rates, readmission rates, or prior auth cycle time give the organization a basis for evaluating whether the deployment succeeded. Vague success criteria lead to vague outcomes.
Build AI literacy across clinical and administrative teams. This does not mean turning nurses into data scientists. It means making sure clinical staff understand what the AI is doing, what it is not doing, and how to recognize when its outputs need human review.
For smaller and rural practices, the calculus is slightly different. Enterprise AI is not the right starting point. SaaS-based ambient scribing and scheduling optimization tools are available at per-user price points that are accessible, require minimal IT infrastructure, and deliver measurable returns within months.
For patients navigating this shifting healthcare landscape and wondering what AI-assisted tools can do for their own health decisions, use Momentary's AI health navigator to explore symptoms, understand conditions, and decide on next steps before booking a visit.
AI in Drug Discovery: Lowering the Billion-Dollar Barrier
Drug development has historically cost an average of $2.6 billion per approved medication, a figure anchored in the cost of failed clinical trials, according to the Tufts Center for the Study of Drug Development. AI is beginning to restructure that cost curve, though it would overstate the current reality to say the savings are yet flowing to patients.
Where AI is making measurable progress is in the early-stage compound screening phase. Traditional drug discovery requires synthesizing thousands of chemical compounds and testing them in biological systems. AI models trained on molecular structures and biological interaction data can now simulate which compounds are most likely to bind to a target protein effectively, reducing the number of physical experiments required by orders of magnitude.
AlphaFold, developed by DeepMind, demonstrated the potential of AI in protein structure prediction and has been cited in subsequent research for accelerating drug target identification. In oncology specifically, AI tools are identifying previously unknown genetic pathways that represent actionable drug targets, which is compressing the pre-clinical discovery timeline from years to months in some programs.
The National Bureau of Economic Research has documented the potential for AI to reduce the cost of bringing new drugs to market, with models suggesting AI-assisted programs could cut pre-clinical and Phase I costs by 30% to 50% for some compound classes. The savings at scale across the pharmaceutical industry would be substantial, though the path from AI-assisted discovery to lower drug prices for patients is not direct and involves pricing, patent, and regulatory dynamics well beyond the scope of AI itself.
The Hidden Costs: Security, Maintenance, and Training
A vendor who quotes only the subscription fee is quoting the beginning of the cost, not the total of it.
HIPAA compliance for AI systems is not a one-time certification. Any AI tool that processes protected health information (PHI) must be covered under a Business Associate Agreement, and the organization deploying it is responsible for ensuring the tool meets HIPAA Security Rule standards for data encryption, access controls, and audit logging. If a vendor hosts models on shared cloud infrastructure without clear PHI isolation, the compliance risk falls on the health system.
Model maintenance is an ongoing expense that is systematically underestimated. AI models trained on data from 2023 begin to drift as clinical practice guidelines update, patient populations shift, and new drug interactions are documented. Retrieval-Augmented Generation (RAG) systems, which ground AI outputs in regularly updated knowledge bases rather than static training data, reduce hallucination risk but require continuous database maintenance and clinical review to ensure the source documents are current and authoritative.
Training staff to work alongside agentic AI is not optional and is not cheap. Effective AI adoption in clinical settings requires training programs, change management support, designated AI champions within clinical teams, and a feedback loop through which frontline staff can report anomalous AI behavior. Organizations that skip this step consistently report lower adoption rates and higher error rates when AI tools do produce incorrect outputs.
Cybersecurity exposure increases with AI adoption. AI systems that interface with EHRs, billing systems, and patient portals expand the attack surface for ransomware and data breaches. The average cost of a healthcare data breach in 2023 reached $10.93 million, the highest of any industry, according to the IBM Cost of a Data Breach Report, and AI integrations must be audited as part of any healthcare organization's cybersecurity program.
The Bottom Line: Is AI Healthcare More Affordable?
The honest answer is: for the system as a whole, yes, over time, if deployed with discipline. For any individual organization deploying AI now, the costs are front-loaded and the savings are back-loaded.
AI increases tech spend. That is not a contingency. It is a structural feature of any meaningful deployment. What AI also does, when implemented well, is shift the healthcare model from expensive reactive treatment toward affordable proactive prevention, and that shift has a multiplier effect on total cost of care.
The clearest economic case for AI in healthcare is not in any single use case. It is in the aggregate: a system where administrative burden is automated, diagnostic errors are caught earlier, high-risk patients are identified before they deteriorate, and fraud is flagged before payment is made. That system costs less per outcome than the one currently operating.
The realistic path to that system runs through rigorous data preparation, honest ROI modeling, balanced vendor evaluation that accounts for hidden costs and risks, and governance frameworks that ensure AI outputs are monitored and accountable.
The question for healthcare operators in 2026 is not whether AI reduces healthcare costs. The evidence says it can. The question is whether a given organization is positioned to capture those savings or whether an AI investment will join the 80% of health AI initiatives that do not achieve their expected outcomes.
Frequently Asked Questions
How much does implementing AI in a hospital actually cost?
Costs range widely by scope and organizational size. A SaaS-based ambient scribing subscription for a small practice runs $500 to $2,000 per provider per month. Mid-market deployments for regional systems, including billing, scheduling, and care management AI, typically land between $200,000 and $800,000 in the first year. Enterprise AI implementations for large health systems or custom clinical AI can reach $500,000 to $5 million or more when data infrastructure, compliance, and change management are fully accounted for.
How much money can AI realistically save in US healthcare?
Estimates from McKinsey and Harvard research put near-term annual savings potential at $200B to $360B, concentrated in administrative functions, prior authorization, fraud detection, and clinical workflow optimization. Morgan Stanley projects the long-range figure could reach $400B to $1.5T by 2050 as AI matures across drug discovery, diagnostics, and population health management.
Does AI in healthcare ever increase costs?
Yes, and this is worth understanding before deployment. AI diagnostic tools with high sensitivity detect more findings, which generates more downstream imaging, biopsies, and procedures. Some of those downstream steps address incidental findings that would never have caused harm, adding cost without improving outcomes. Additionally, AI billing optimization and AI-powered claims denial create an arms race between providers and payers where both sides spend on AI without the patient benefiting.
Why do so many AI healthcare projects fail to deliver expected savings?
Approximately 80% of health AI initiatives do not achieve their projected outcomes. The most common failure modes are data quality problems at the source EHR level, clinical workflows that are designed around AI tools rather than into them, insufficient governance to detect model drift over time, and change management gaps that leave clinical staff working around AI rather than with it.
What is agentic AI and why does it matter for healthcare costs?
Agentic AI refers to systems that execute multi-step workflows autonomously, rather than performing single tasks in isolation. In healthcare, this means AI that handles an entire prior authorization process end-to-end, or an AI that manages patient follow-up across a care journey without staff involvement at each step. Agentic AI has higher ROI potential per deployed use case than traditional task-specific AI, but also higher implementation complexity and more significant failure consequences if the system malfunctions.
Can AI replace physicians?
No. AI tools currently approved and deployed in US healthcare settings are designed to support clinical decision-making, not replace it. They reduce documentation burden, flag diagnostic anomalies, and automate administrative workflows. The clinical judgment required for diagnosis, treatment planning, and patient communication remains a physician and care team function. Regulatory frameworks, liability standards, and the complexity of medicine as practiced across real patient populations make AI a tool for clinicians, not a substitute for them.
References
- PMC/NLM: AI and Healthcare Cost Effectiveness — Cited for data preparation consuming 60-80% of AI project time, and McKinsey/Harvard savings projections.
- Morgan Stanley: AI in Healthcare May Save Trillions by 2050 — Cited for $400B to $1.5T long-range AI savings projection.
- NBER Working Paper on AI and Drug Discovery — Cited for AI potential to reduce pre-clinical and Phase I drug development costs by 30-50%.
- Frontiers: Leveraging AI and Machine Learning for Healthcare Cost Effectiveness — Cited for 80% AI health initiative failure rate.
- PMC Article on AI Implementation — Cited for structural barriers to AI adoption in health systems.
- PMC Article on Agentic AI in Healthcare — Cited for agentic AI growth trajectory and ambient scribe market sizing.
- PubMed: AI Healthcare Outcomes Analysis — Cited for clinical AI performance benchmarks.
- PMC Article on AI Savings by Stakeholder — Cited for stakeholder-segmented AI savings ranges.
- University of Pennsylvania LDI: US AI Boom Could Cause Health Care Costs to Soar — Cited for risks of care cascade inflation and cost-of-care dynamics under fee-for-service models.



